

Major alterations in the mononuclear phagocyte landscape associated with COVID-19 severity
- PMID: 33479167
- PMCID: PMC8017719
- DOI: 10.1073/pnas.2018587118
Major alterations in the mononuclear phagocyte landscape associated with COVID-19 severity
Abstract
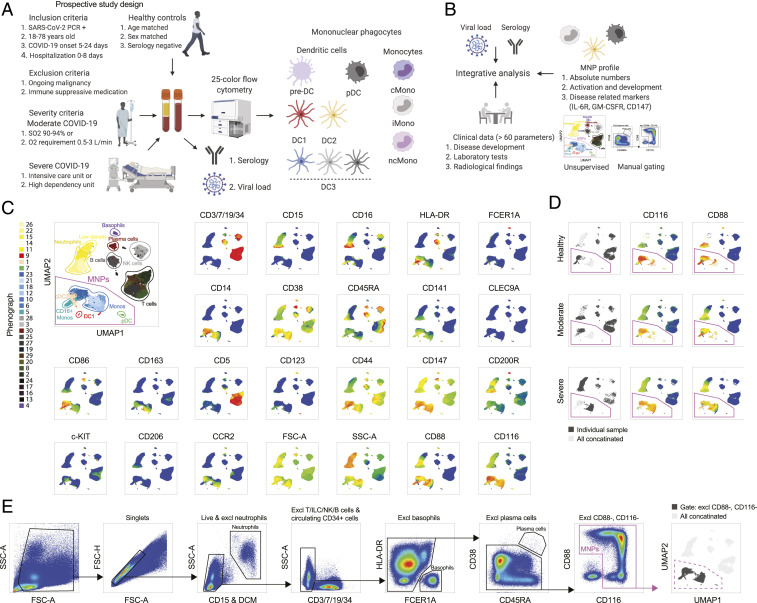
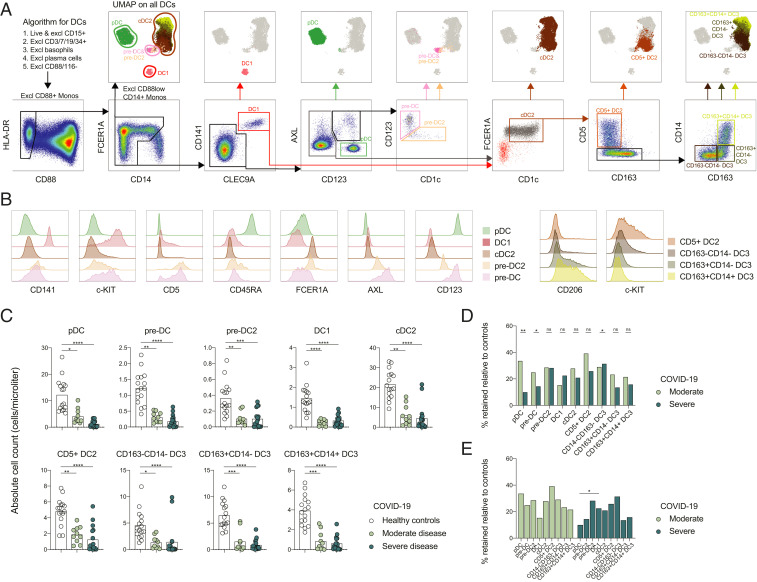
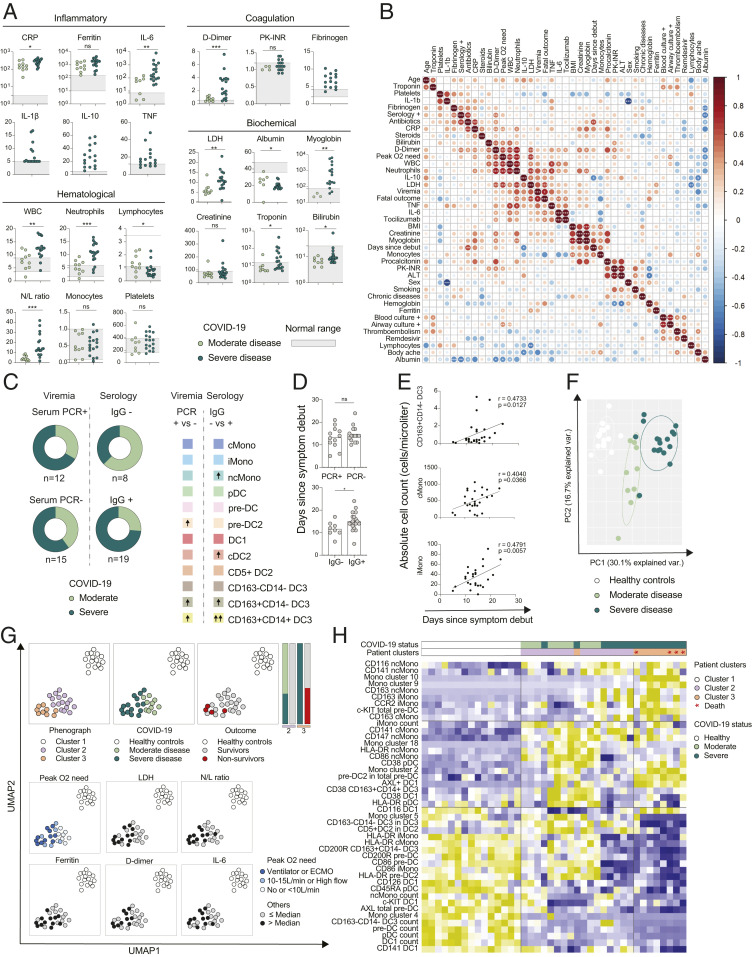
Dendritic cells (DCs) and monocytes are crucial mediators of innate and adaptive immune responses during viral infection, but misdirected responses by these cells may contribute to immunopathology. Here, we performed high-dimensional flow cytometry-analysis focusing on mononuclear phagocyte (MNP) lineages in SARS-CoV-2-infected patients with moderate and severe COVID-19. We provide a deep and comprehensive map of the MNP landscape in COVID-19. A redistribution of monocyte subsets toward intermediate monocytes and a general decrease in circulating DCs was observed in response to infection. Severe disease coincided with the appearance of monocytic myeloid-derived suppressor cell-like cells and a higher frequency of pre-DC2. Furthermore, phenotypic alterations in MNPs, and their late precursors, were cell-lineage-specific and associated either with the general response against SARS-CoV-2 or COVID-19 severity. This included an interferon-imprint in DC1s observed in all patients and a decreased expression of the coinhibitory molecule CD200R in pre-DCs, DC2s, and DC3 subsets of severely sick patients. Finally, unsupervised analysis revealed that the MNP profile, alone, pointed to a cluster of COVID-19 nonsurvivors. This study provides a reference for the MNP response to SARS-CoV-2 infection and unravels mononuclear phagocyte dysregulations associated with severe COVID-19.
Keywords: COVID-19; DCs; monocytes; pre-DCs.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
The authors declare no competing interest.
Figures



References
-
- Rescigno M., Dendritic cell functions: Learning from microbial evasion strategies. Semin. Immunol. 27, 119–124 (2015). - PubMed
-
- Wong K. L., et al., Gene expression profiling reveals the defining features of the classical, intermediate, and nonclassical human monocyte subsets. Blood 118, e16–e31 (2011). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
