

Ex vivo culture of intact human patient derived pancreatic tumour tissue
- PMID: 33479301
- PMCID: PMC7820421
- DOI: 10.1038/s41598-021-81299-0
Ex vivo culture of intact human patient derived pancreatic tumour tissue
Abstract
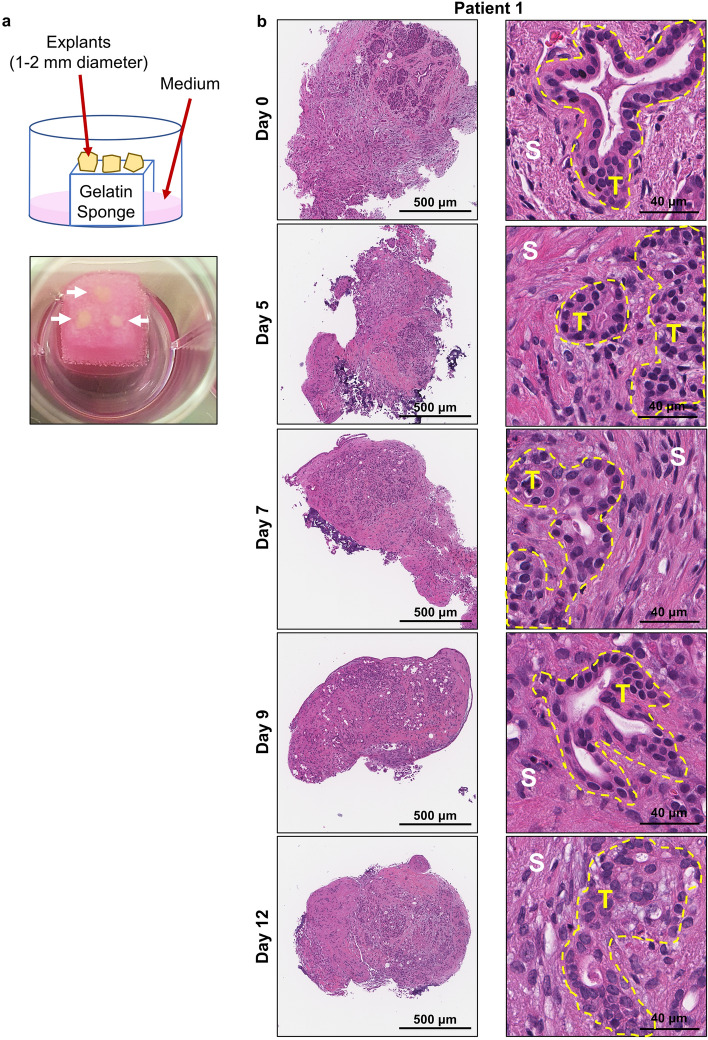
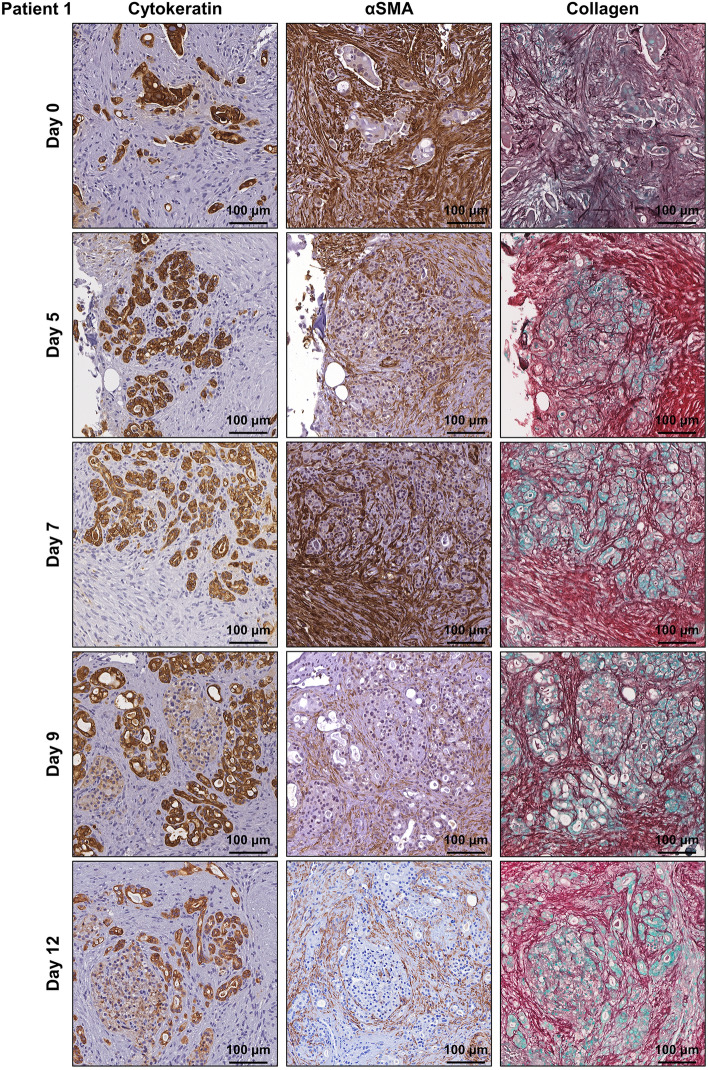
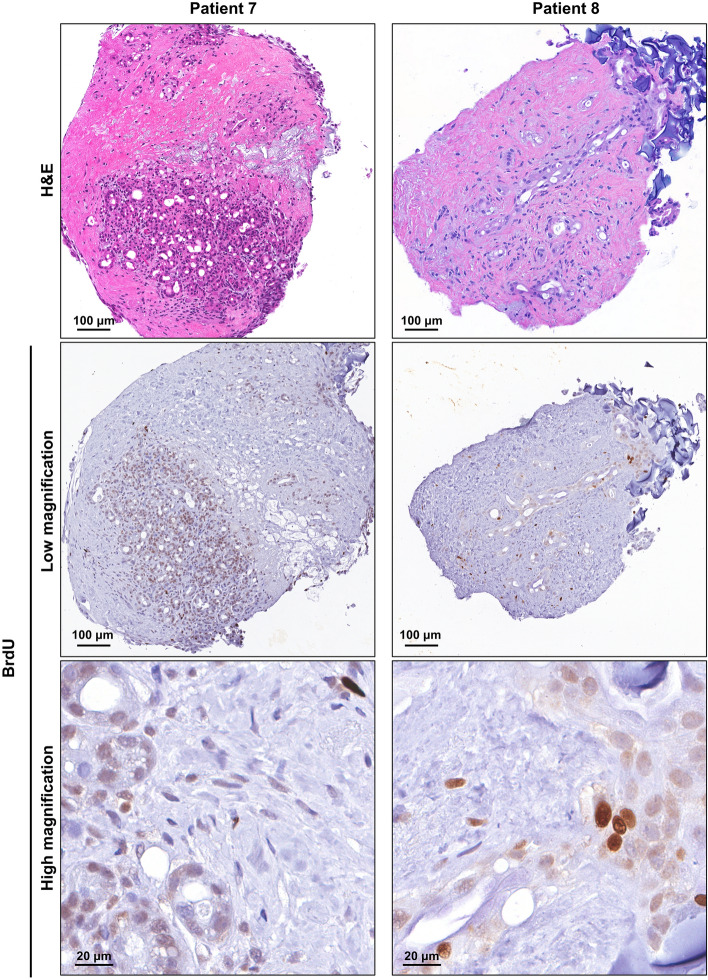
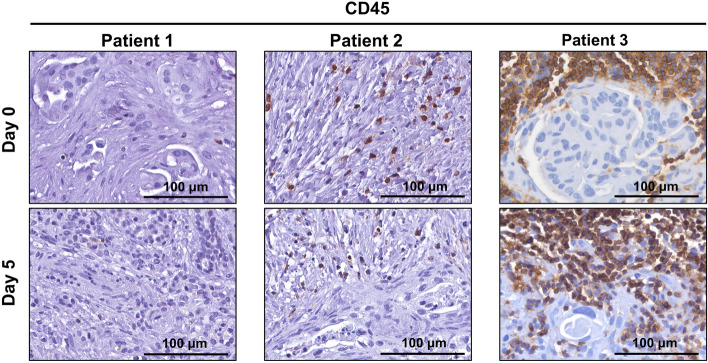
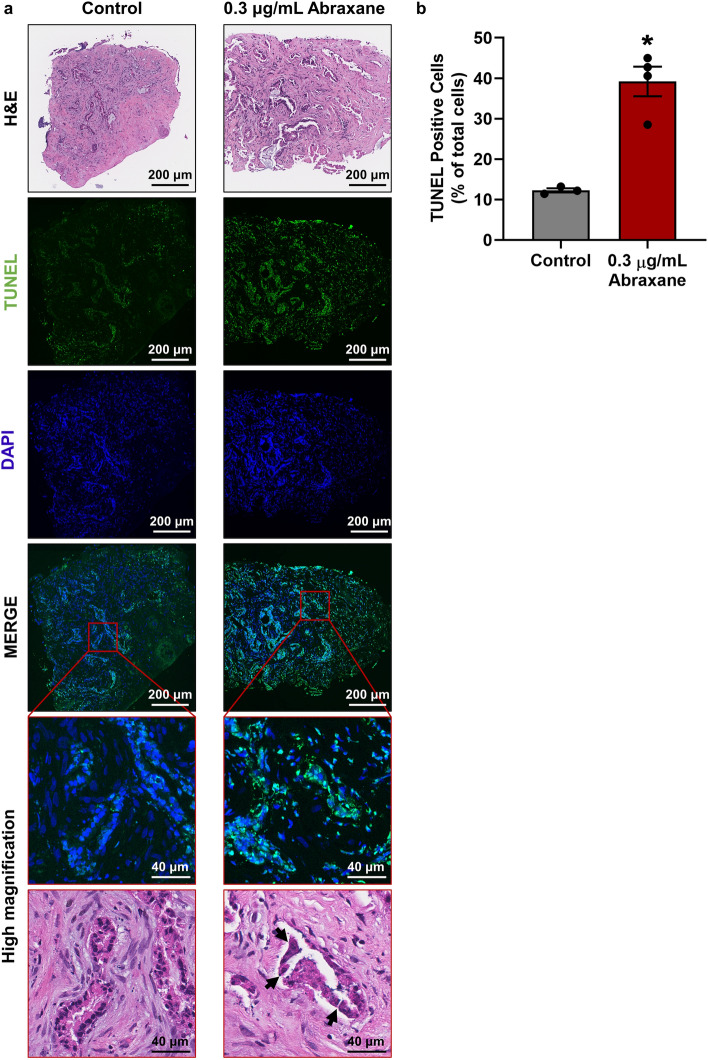
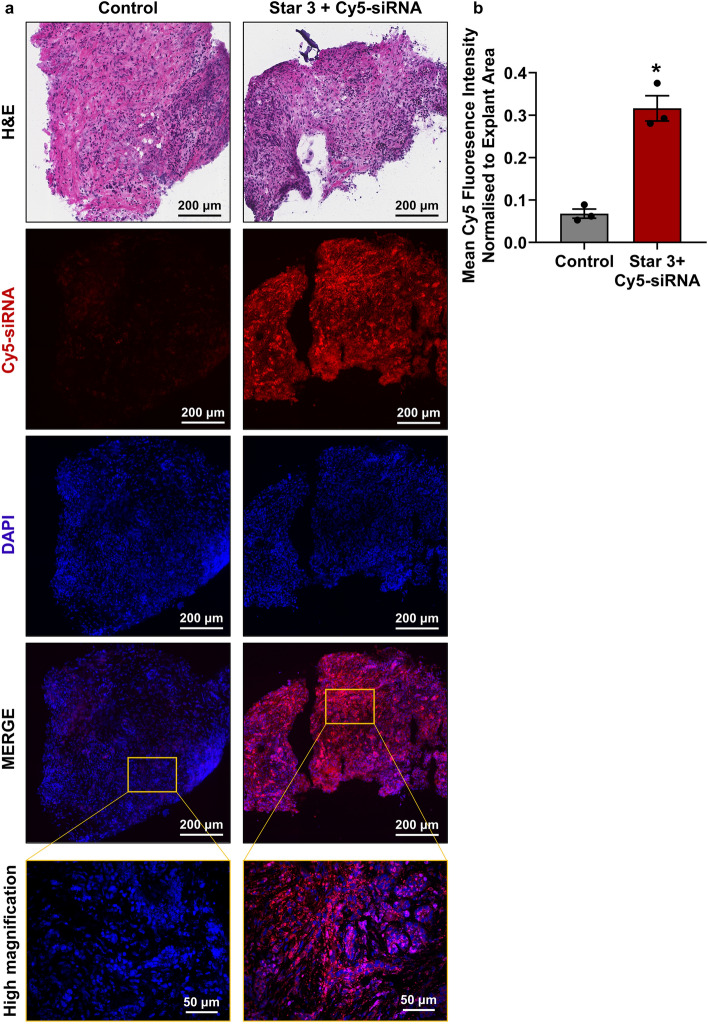
The poor prognosis of pancreatic ductal adenocarcinoma (PDAC) is attributed to the highly fibrotic stroma and complex multi-cellular microenvironment that is difficult to fully recapitulate in pre-clinical models. To fast-track translation of therapies and to inform personalised medicine, we aimed to develop a whole-tissue ex vivo explant model that maintains viability, 3D multicellular architecture, and microenvironmental cues of human pancreatic tumours. Patient-derived surgically-resected PDAC tissue was cut into 1-2 mm explants and cultured on gelatin sponges for 12 days. Immunohistochemistry revealed that human PDAC explants were viable for 12 days and maintained their original tumour, stromal and extracellular matrix architecture. As proof-of-principle, human PDAC explants were treated with Abraxane and we observed different levels of response between patients. PDAC explants were also transfected with polymeric nanoparticles + Cy5-siRNA and we observed abundant cytoplasmic distribution of Cy5-siRNA throughout the PDAC explants. Overall, our novel model retains the 3D architecture of human PDAC and has advantages over standard organoids: presence of functional multi-cellular stroma and fibrosis, and no tissue manipulation, digestion, or artificial propagation of organoids. This provides unprecedented opportunity to study PDAC biology including tumour-stromal interactions and rapidly assess therapeutic response to drive personalised treatment.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- Phillips, P. in Pancreatic Cancer and Tumour Microenvironment (ed Trivandrum) Chap. 3 (Transworld Research Network, 2012). - PubMed
Publication types
MeSH terms
Grants and funding
- RSP-011-18/19/Tour de Cure PhD Support Scholarship
- RSP-011-18/19/Tour de Cure PhD Support Scholarship
- RSP-011-18/19/Tour de Cure PhD Support Scholarship
- APCF0050618/Avner Pancreatic Cancer Foundation Innovation Grant
- APCF0050618/Avner Pancreatic Cancer Foundation Innovation Grant
- APCF0050618/Avner Pancreatic Cancer Foundation Innovation Grant
- APCF0050618/Avner Pancreatic Cancer Foundation Innovation Grant
- CDF181166/Cancer-Institute NSW ECF/CDF
- APP1136974/NHMRC Senior Research Fellowship
- PRF1117/Beat Cancer Project Principal Cancer Research Fellowship
- 2017/AWD002/Cancer Institute NSW 'The Professor Rob Sutherland AO Make a Difference Award'
- APP1144108/NHMRC project grant
- APP1144108/NHMRC project grant
- APP1144108/NHMRC project grant
- APP1126736/Cancer Australia
- APP1126736/Cancer Australia
- APP1126736/Cancer Australia
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
