

Deep learning predicts postsurgical recurrence of hepatocellular carcinoma from digital histopathologic images
- PMID: 33479370
- PMCID: PMC7820423
- DOI: 10.1038/s41598-021-81506-y
Deep learning predicts postsurgical recurrence of hepatocellular carcinoma from digital histopathologic images
Abstract
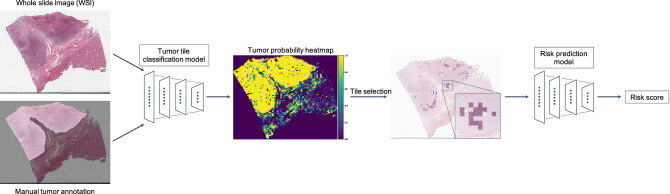
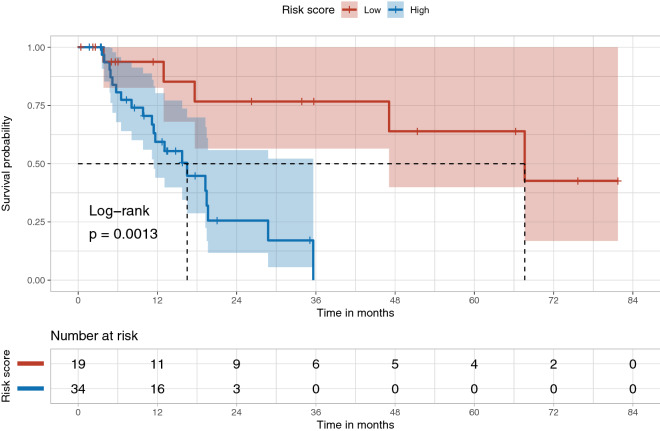
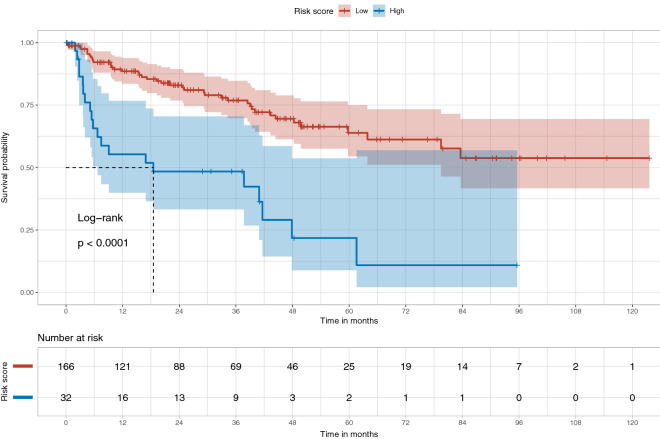
Recurrence risk stratification of patients undergoing primary surgical resection for hepatocellular carcinoma (HCC) is an area of active investigation, and several staging systems have been proposed to optimize treatment strategies. However, as many as 70% of patients still experience tumor recurrence at 5 years post-surgery. We developed and validated a deep learning-based system (HCC-SurvNet) that provides risk scores for disease recurrence after primary resection, directly from hematoxylin and eosin-stained digital whole-slide images of formalin-fixed, paraffin embedded liver resections. Our model achieved concordance indices of 0.724 and 0.683 on the internal and external test cohorts, respectively, exceeding the performance of the standard Tumor-Node-Metastasis classification system. The model's risk score stratified patients into low- and high-risk subgroups with statistically significant differences in their survival distributions, and was an independent risk factor for post-surgical recurrence in both test cohorts. Our results suggest that deep learning-based models can provide recurrence risk scores which may augment current patient stratification methods and help refine the clinical management of patients undergoing primary surgical resection for HCC.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Brierley J, Gospodarowicz MK, Wittekind C, editors. Liver in TNM Classification of Malignant Tumours. New York: Wiley; 2017. pp. 80–84.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
