

Expanding the Treatment Landscape for Lennox-Gastaut Syndrome: Current and Future Strategies
- PMID: 33479851
- PMCID: PMC7873005
- DOI: 10.1007/s40263-020-00784-8
Expanding the Treatment Landscape for Lennox-Gastaut Syndrome: Current and Future Strategies
Abstract
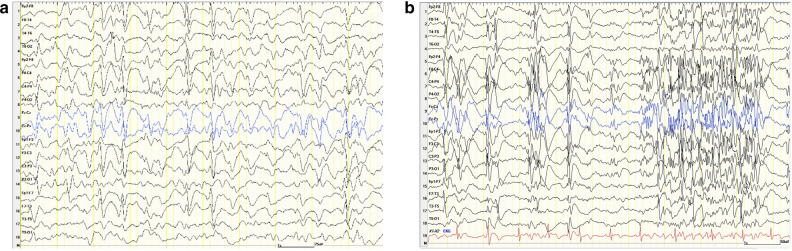
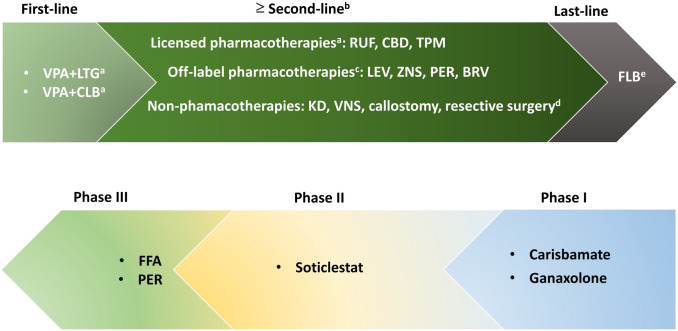
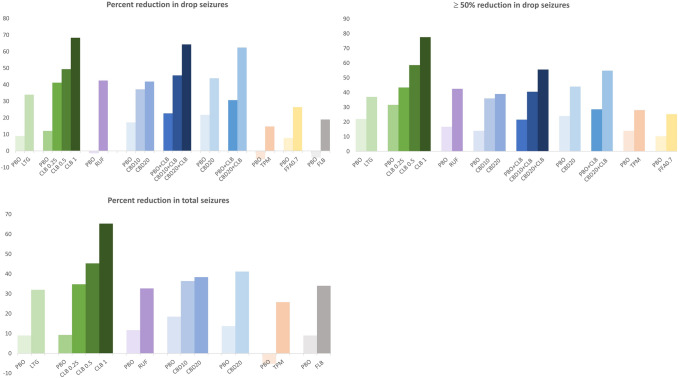
Lennox-Gastaut syndrome (LGS), a childhood-onset severe developmental and epileptic encephalopathy (DEE), is an entity that encompasses a heterogenous group of aetiologies, with no single genetic cause. It is characterised by multiple seizure types, an abnormal EEG with generalised slow spike and wave discharges and cognitive impairment, associated with high morbidity and profound effects on the quality of life of patients and their families. Drug-refractory seizures are a hallmark and treatment is further complicated by its multiple morbidities, which evolve over the patient's lifetime. This review provides a comprehensive overview of the current and future options for the treatment of seizures associated with LGS. Six treatments are specifically indicated as adjunct therapies for the treatment of seizures associated with LGS in the US: lamotrigine, clobazam, rufinamide, topiramate, felbamate and most recently cannabidiol. These therapies have demonstrated reductions in drop seizures in 15%-68% of patients across trials, with responder rates (≥ 50% reduction in drop seizures) of 37%-78%. Valproate is still the preferred first-line treatment, generally in combination with lamotrigine or clobazam. Other treatments frequently used off-label include the broad spectrum anti-epileptic drugs (AED) levetiracetam, zonisamide and perampanel, while recent evidence from observational studies has indicated that a newer AED, the levetiracetam analogue brivaracetam, may be effective and well tolerated in LGS patients. Other treatments in clinical development include fenfluramine in late phase III, perampanel, soticlestat-OV953/TAK-953, carisbamate and ganaxolone. Non-pharmacologic interventions include the ketogenic diet, vagus nerve stimulation and surgical interventions; these are also expanding, with the potential for less invasive techniques for corpus callosotomy that have promise for reducing complications. However, despite these advancements, patients continue to experience a significant burden. Because LGS is not a single entity, tailoring of treatment is needed as opposed to a 'one size fits all' approach. Further research is needed into the underlying aetiologies and pathophysiology of LGS, together with advancements in treatments that encompass the spectrum of seizures associated with this complex syndrome.
Conflict of interest statement
A. Strzelczyk reports personal fees and grants from Arvelle Therapeutics, Desitin Arzneimittel, Eisai, GW Pharmaceuticals, LivaNova, Marinus Pharmaceuticals, Medtronic, UCB Pharma and Zogenix. S. Schubert-Bast reports personal fees from Eisai, Desitin Pharma, GW Pharmaceuticals, LivaNova, UCB Pharma and Zogenix.
Figures

References
-
- Crespel A, Gelisse P, Macorig G, Nikanorova M, Ferlazzo E, Genton P, et al. Lennox-Gastaut syndrome. In: Bureau M, Genton P, Dravet C, Delgado-Escueta AV, Guerrini R, Tassinari CA, et al., editors. Epileptic syndromes in infancy, childhood and adolescence. 6. Arcueil: John Libbey Eurotext; 2019.
-
- Cuomo A, Riel-Romero RM. Lennox gastaut syndrome. Treasure Island: StatPearls Publishing; 2020. - PubMed
-
- Arzimanoglou A, French J, Blume WT, Cross JH, Ernst JP, Feucht M, et al. Lennox-Gastaut syndrome: a consensus approach on diagnosis, assessment, management, and trial methodology. Lancet Neurol. 2009;8(1):82–93. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
