

An Automated Deep Learning Method for Tile AO/OTA Pelvic Fracture Severity Grading from Trauma whole-Body CT
- PMID: 33479859
- PMCID: PMC7886919
- DOI: 10.1007/s10278-020-00399-x
An Automated Deep Learning Method for Tile AO/OTA Pelvic Fracture Severity Grading from Trauma whole-Body CT
Abstract
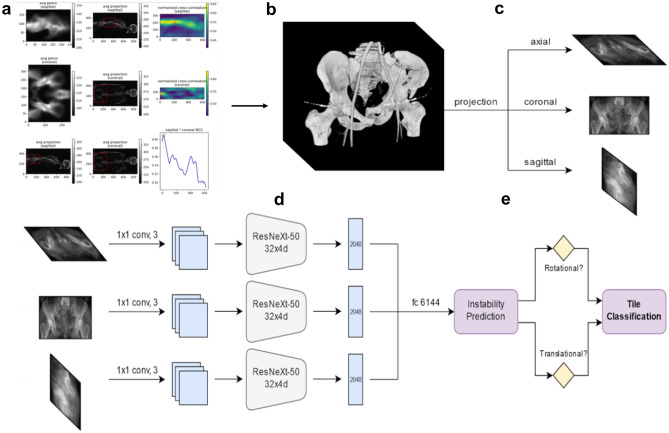
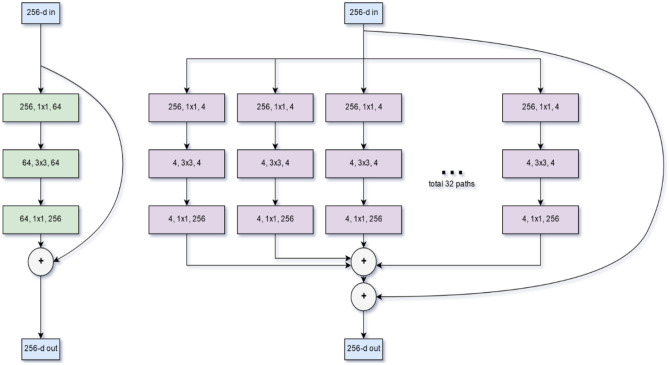
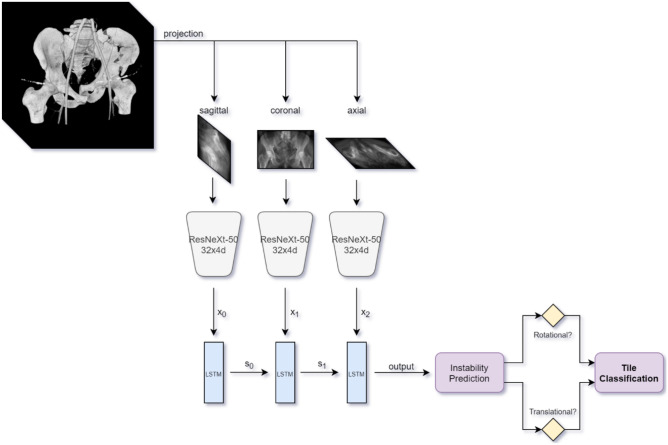
Admission trauma whole-body CT is routinely employed as a first-line diagnostic tool for characterizing pelvic fracture severity. Tile AO/OTA grade based on the presence or absence of rotational and translational instability corresponds with need for interventions including massive transfusion and angioembolization. An automated method could be highly beneficial for point of care triage in this critical time-sensitive setting. A dataset of 373 trauma whole-body CTs collected from two busy level 1 trauma centers with consensus Tile AO/OTA grading by three trauma radiologists was used to train and test a triplanar parallel concatenated network incorporating orthogonal full-thickness multiplanar reformat (MPR) views as input with a ResNeXt-50 backbone. Input pelvic images were first derived using an automated registration and cropping technique. Performance of the network for classification of rotational and translational instability was compared with that of (1) an analogous triplanar architecture incorporating an LSTM RNN network, (2) a previously described 3D autoencoder-based method, and (3) grading by a fourth independent blinded radiologist with trauma expertise. Confusion matrix results were derived, anchored to peak Matthews correlation coefficient (MCC). Associations with clinical outcomes were determined using Fisher's exact test. The triplanar parallel concatenated method had the highest accuracies for discriminating translational and rotational instability (85% and 74%, respectively), with specificity, recall, and F1 score of 93.4%, 56.5%, and 0.63 for translational instability and 71.7%, 75.7%, and 0.77 for rotational instability. Accuracy of this method was equivalent to the single radiologist read for rotational instability (74.0% versus 76.7%, p = 0.40), but significantly higher for translational instability (85.0% versus 75.1, p = 0.0007). Mean inference time was < 0.1 s per test image. Translational instability determined with this method was associated with need for angioembolization and massive transfusion (p = 0.002-0.008). Saliency maps demonstrated that the network focused on the sacroiliac complex and pubic symphysis, in keeping with the AO/OTA grading paradigm. A multiview concatenated deep network leveraging 3D information from orthogonal thick-MPR images predicted rotationally and translationally unstable pelvic fractures with accuracy comparable to an independent reader with trauma radiology expertise. Model output demonstrated significant association with key clinical outcomes.
Keywords: Convolutional neural network; Deep learning; Pelvic fracture; Pelvic instability; Pelvic ring disruption; Tile classification.
Figures
References
-
- Garlapati AK, Ashwood N. An overview of pelvic ring disruption. Trauma 14(2):169-178,2012
-
- Raniga SB, Mittal AK, Bernstein M, Skalski MR, Al-Hadidi AM. Multidetector CT in Vascular Injuries Resulting from Pelvic Fractures: A Primer for Diagnostic Radiologists. RadioGraphics 39(7):2111-2129,2019 - PubMed
-
- Vaidya R, Scott AN, Tonnos F, Hudson I, Martin AJ, Sethi A. Patients with pelvic fractures from blunt trauma. What is the cause of mortality and when? Am J Surg 211(3):495–500,2016 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
