

Hospital-Level Care at Home for Acutely Ill Adults: a Qualitative Evaluation of a Randomized Controlled Trial
- PMID: 33479931
- PMCID: PMC8298744
- DOI: 10.1007/s11606-020-06416-7
Hospital-Level Care at Home for Acutely Ill Adults: a Qualitative Evaluation of a Randomized Controlled Trial
Abstract
Background: Substitutive hospital-level care in a patient's home ("home hospital") has been shown to lower cost, utilization, and readmission compared to traditional hospital care. However, patients' perspectives to help explain how and why interventions like home hospital accomplish many of these results are lacking.
Objective: Elucidate and explain patient perceptions of home hospital versus traditional hospital care to better describe the different perceptions of care in both settings.
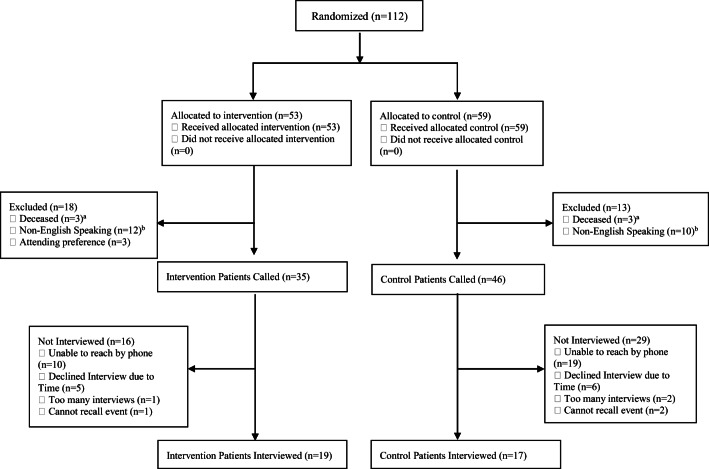
Design: Qualitative evaluation of a randomized controlled trial.
Participants: 36 hospitalized patients (19 home; 17 control).
Intervention: Traditional hospital ("control") versus home hospital ("home"), including nurse and physician home visits, intravenous medications, remote monitoring, video communication, and point-of-care testing.
Approach: We conducted a thematic content analysis of semi-structured interviews. Team members developed a coding structure through a multiphase approach, utilizing a constant comparative method.
Key results: Themes clustered around 3 domains: clinician factors, factors promoting healing, and systems factors. Clinician factors were similar in both groups; both described beneficial interactions with clinical staff; however, home patients identified greater continuity of care. For factors promoting healing, home patients described a locus of control surrounding their sleep, activity, and environmental comfort that control patients lacked. For systems factors, home patients experienced more efficient processes and logistics, particularly around admission and technology use, while both noted difficulty with discharge planning.
Conclusions: Compared to control patients, home patients had better experiences with their care team, had more experiences promoting healing such as better sleep and physical activity, and had better experiences with systems factors such as the admission processes. Potential explanations include continuity of care, the power and familiarity of the home, and streamlined logistics. Future improvements include enhanced care transitions and ensuring digital interfaces are usable.
Trial registration: NCT03203759.
Keywords: home hospital; home-based care; hospital alternative; hospital at home; hospital experience; qualitative.
© 2021. Society of General Internal Medicine.
Conflict of interest statement
Dr. Levine is a recipient of funding from Biofourmis for an investigator-initiated study of machine learning warning scores for acutely ill patients, both traditionally and home hospitalized.
Dr. Schnipper is a recipient of funding from Mallinckrodt Pharmaceuticals for an investigator-initiated study of opioid-related adverse drug events in post-operative hospitalized patients.
All other authors declare that they do not have a conflict of interest.
Figures
References
-
- FastStats - Health Expenditures. Accessed December 3, 2018. https://www.cdc.gov/nchs/fastats/health-expenditures.htm
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
