

Classification and Prediction of Post-Trauma Outcomes Related to PTSD Using Circadian Rhythm Changes Measured via Wrist-Worn Research Watch in a Large Longitudinal Cohort
- PMID: 33481725
- PMCID: PMC8395207
- DOI: 10.1109/JBHI.2021.3053909
Classification and Prediction of Post-Trauma Outcomes Related to PTSD Using Circadian Rhythm Changes Measured via Wrist-Worn Research Watch in a Large Longitudinal Cohort
Abstract
Post-Traumatic Stress Disorder (PTSD) is a psychiatric condition resulting from threatening or horrifying events. We hypothesized that circadian rhythm changes, measured by a wrist-worn research watch are predictive of post-trauma outcomes.
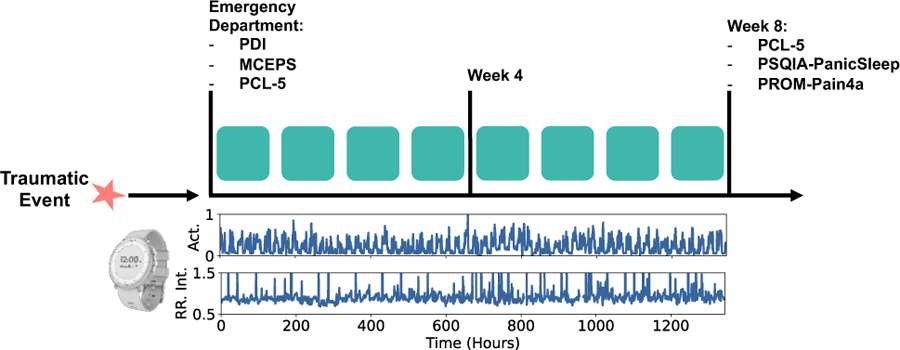
Approach: 1618 post-trauma patients were enrolled after admission to emergency departments (ED). Three standardized questionnaires were administered at week eight to measure post-trauma outcomes related to PTSD, sleep disturbance, and pain interference with daily life. Pulse activity and movement data were captured from a research watch for eight weeks. Standard and novel movement and cardiovascular metrics that reflect circadian rhythms were derived using this data. These features were used to train different classifiers to predict the three outcomes derived from week-eight surveys. Clinical surveys administered at ED were also used as features in the baseline models.
Results: The highest cross-validated performance of research watch-based features was achieved for classifying participants with pain interference by a logistic regression model, with an area under the receiver operating characteristic curve (AUC) of 0.70. The ED survey-based model achieved an AUC of 0.77, and the fusion of research watch and ED survey metrics improved the AUC to 0.79.
Significance: This work represents the first attempt to predict and classify post-trauma symptoms from passive wearable data using machine learning approaches that leverage the circadian desynchrony in a potential PTSD population.
Figures






References
-
- American Psychiatric Association and others, Diagnostic and statistical manual of mental disorders DSM-5, American Psychiatric Pub, 2013.
-
- Sharp TJ and Harvey AG, “Chronic pain and posttraumatic stress disorder: mutual maintenance?,” Clinical Psychology Review, vol. 21, no. 6, pp. 857–877, 2001. - PubMed
-
- Fishbain DA, Pulikal A, Lewis JE and Gao J, “Chronic pain types differ in their reported prevalence of post-traumatic stress disorder (PTSD) and there is consistent evidence that chronic pain is associated with PTSD: an evidence-based structured systematic review,” Pain Medicine, vol. 18, no. 4, pp. 711–735, 2017. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
