

Usage and Weekly Attrition in a Smartphone-Based Health Behavior Intervention for Adolescents: Pilot Randomized Controlled Trial
- PMID: 33481750
- PMCID: PMC7929738
- DOI: 10.2196/21432
Usage and Weekly Attrition in a Smartphone-Based Health Behavior Intervention for Adolescents: Pilot Randomized Controlled Trial
Abstract
Background: The majority of adolescents own smartphones, although only 8% of them use health apps. Attrition rates from adolescent mobile health (mHealth) interventions for treating mental health problems such as anxiety and depression are an issue with a high degree of variation. Attrition in mHealth interventions targeting adolescent populations is frequently presented in a two-point fashion, from initiation of the intervention to the end of treatment, lacking more time-specific information on usage and times of attrition. Self-efficacy could provide an avenue to lower attrition rates, although a better understanding of the relationship between mental health factors and time-specific attrition rates is needed.
Objective: The aims of this study were to obtain time-specific attrition rates among adolescents in an mHealth intervention, and to describe the intervention's usage and feasibility in relation to adolescent self-efficacy levels, and emotional and physical health.
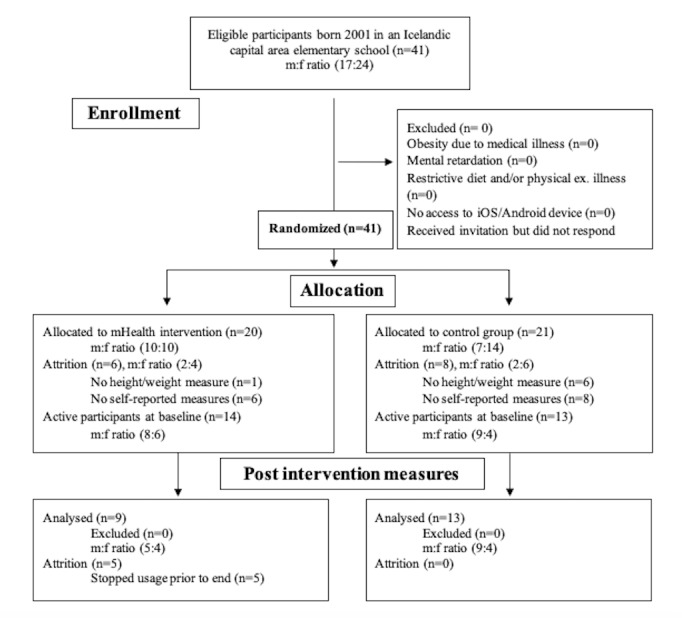
Methods: A single-center randomized controlled public school pilot trial was undertaken with 41 adolescents. Outcome measures were assessed at baseline and after 6 weeks, while in-app activity and attrition rates were continually assessed throughout the intervention period. The primary outcome was attrition based on time and type of in-app health behavior usage, and feasibility of the mHealth app. Secondary outcome measures were self-efficacy levels, depressive and anxiety symptoms, as well as standardized BMI and sleep. Analyses of group mean variances with adjusted α levels through Bonferroni corrections were used to assess main outcome effects.
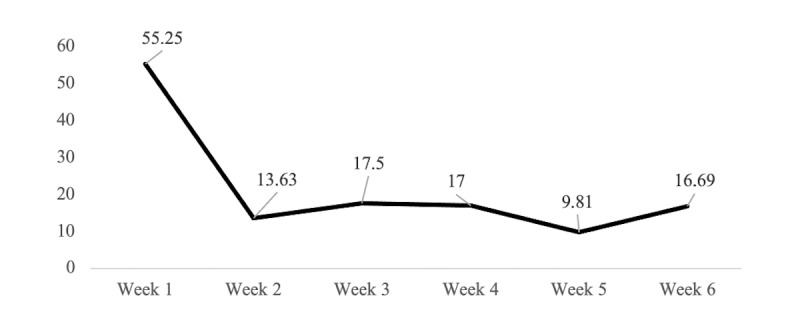
Results: The attrition from initiation of the intervention to 6-week follow up was 35%. Attrition started in the third week of the intervention and was related to daily time of app usage (Rt=0.43, P<.001). The number of average weekly in-app health exercises completed decreased significantly from the first week of the intervention (mean 55.25, SD 10.96) to the next week (mean 13.63, SD 2.94). However, usage increased by 22% between week 2 and the last week of the intervention (mean 16.69, SD 8.37). Usability measures revealed satisfactory scores (mean 78.09, SD 9.82) without gender differences (P=.85). Self-reported daily physical activity increased by 19.61% in the intervention group but dropped by 26.21% among controls. Self-efficacy levels increased by 8.23% in the invention arm compared to a 3.03% decrease in the control group.
Conclusions: This pilot study demonstrated the feasibility and usability of an mHealth intervention among adolescent participants. Indications were toward beneficial effects on physical and mental health that warrant further research. Focus on time-specific attrition measures alongside daily times of usage and ways to increase participants' self-efficacy levels appear to be a promising avenue for research on mHealth interventions for adolescent populations with the aim to ultimately lower attrition rates.
Keywords: adolescent; attrition; behavior; intervention; mHealth; mental health; physical activity; self-efficacy; young adult.
©Erlendur Egilsson, Ragnar Bjarnason, Urdur Njardvik. Originally published in JMIR Formative Research (http://formative.jmir.org), 17.02.2021.
Conflict of interest statement
Conflicts of Interest: EE is a minority shareholder and former employee of SidekickHealth AB. The other authors have no conflicts of interest to declare.
Figures
Similar articles
-
Usage and Daily Attrition of a Smartphone-Based Health Behavior Intervention: Randomized Controlled Trial.JMIR Mhealth Uhealth. 2023 Jun 26;11:e45414. doi: 10.2196/45414. JMIR Mhealth Uhealth. 2023. PMID: 37358888 Free PMC article. Clinical Trial.
-
Apps for IMproving FITness and Increasing Physical Activity Among Young People: The AIMFIT Pragmatic Randomized Controlled Trial.J Med Internet Res. 2015 Aug 27;17(8):e210. doi: 10.2196/jmir.4568. J Med Internet Res. 2015. PMID: 26316499 Free PMC article. Clinical Trial.
-
Mobile Health Apps in Pediatric Obesity Treatment: Process Outcomes From a Feasibility Study of a Multicomponent Intervention.JMIR Mhealth Uhealth. 2020 Jul 8;8(7):e16925. doi: 10.2196/16925. JMIR Mhealth Uhealth. 2020. PMID: 32673267 Free PMC article. Clinical Trial.
-
User Engagement With Smartphone Apps and Cardiovascular Disease Risk Factor Outcomes: Systematic Review.JMIR Cardio. 2021 Feb 3;5(1):e18834. doi: 10.2196/18834. JMIR Cardio. 2021. PMID: 33533730 Free PMC article. Review.
-
Novel Augmentation Strategies in Major Depression.Dan Med J. 2017 Apr;64(4):B5338. Dan Med J. 2017. PMID: 28385173 Review.
Cited by
-
Personalized mood prediction from patterns of behavior collected with smartphones.NPJ Digit Med. 2024 Feb 28;7(1):49. doi: 10.1038/s41746-024-01035-6. NPJ Digit Med. 2024. PMID: 38418551 Free PMC article.
-
Effectiveness of mHealth App-Based Interventions for Increasing Physical Activity and Improving Physical Fitness in Children and Adolescents: Systematic Review and Meta-Analysis.JMIR Mhealth Uhealth. 2024 Apr 30;12:e51478. doi: 10.2196/51478. JMIR Mhealth Uhealth. 2024. PMID: 38687568 Free PMC article.
-
Mobile apps to reduce depressive symptoms and alcohol use in youth: A systematic review and meta-analysis: A systematic review.Campbell Syst Rev. 2024 Apr 26;20(2):e1398. doi: 10.1002/cl2.1398. eCollection 2024 Jun. Campbell Syst Rev. 2024. PMID: 38680950 Free PMC article. Review.
-
Nonusage Attrition of Adolescents in an mHealth Promotion Intervention and the Role of Socioeconomic Status: Secondary Analysis of a 2-Arm Cluster-Controlled Trial.JMIR Mhealth Uhealth. 2022 May 10;10(5):e36404. doi: 10.2196/36404. JMIR Mhealth Uhealth. 2022. PMID: 35536640 Free PMC article. Clinical Trial.
-
The Impact of Mobile Technology-Delivered Interventions on Youth Well-being: Systematic Review and 3-Level Meta-analysis.JMIR Ment Health. 2022 Jul 29;9(7):e34254. doi: 10.2196/34254. JMIR Ment Health. 2022. PMID: 35904845 Free PMC article. Review.
References
-
- Erskine HE, Baxter AJ, Patton G, Moffitt TE, Patel V, Whiteford HA, Scott JG. The global coverage of prevalence data for mental disorders in children and adolescents. Epidemiol Psychiatr Sci. 2017 Aug;26(4):395–402. doi: 10.1017/S2045796015001158. http://europepmc.org/abstract/MED/26786507 - DOI - PMC - PubMed
-
- Philipp J, Zeiler M, Waldherr K, Truttmann S, Dür W, Karwautz AFK, Wagner G. Prevalence of emotional and behavioral problems and subthreshold psychiatric disorders in Austrian adolescents and the need for prevention. Soc Psychiatry Psychiatr Epidemiol. 2018 Dec;53(12):1325–1337. doi: 10.1007/s00127-018-1586-y. http://europepmc.org/abstract/MED/30159723 - DOI - PMC - PubMed
-
- Data and Statistics on Childrens Mental Health. Centers for Disease Control and Prevention (CDC) 2020. Jun 15, [2020-06-21]. https://www.cdc.gov/childrensmentalhealth/data.html.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
