

Prism adaptation treatment to address spatial neglect in an intensive rehabilitation program: A randomized pilot and feasibility trial
- PMID: 33481828
- PMCID: PMC7822563
- DOI: 10.1371/journal.pone.0245425
Prism adaptation treatment to address spatial neglect in an intensive rehabilitation program: A randomized pilot and feasibility trial
Abstract
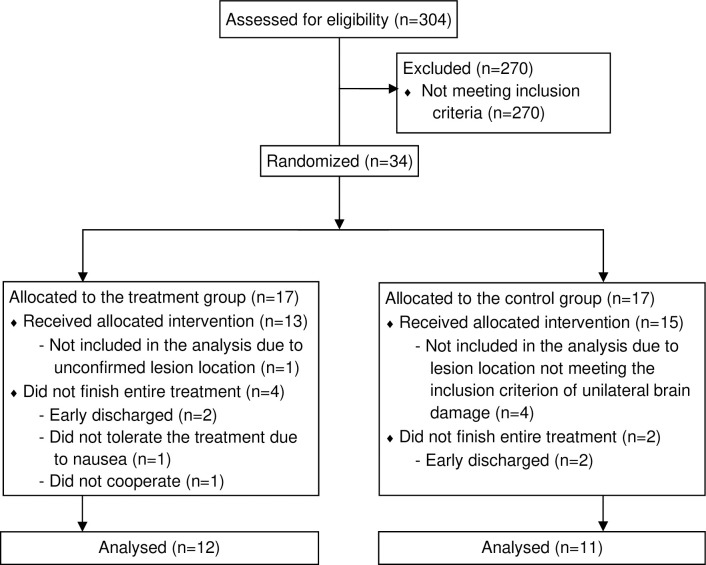
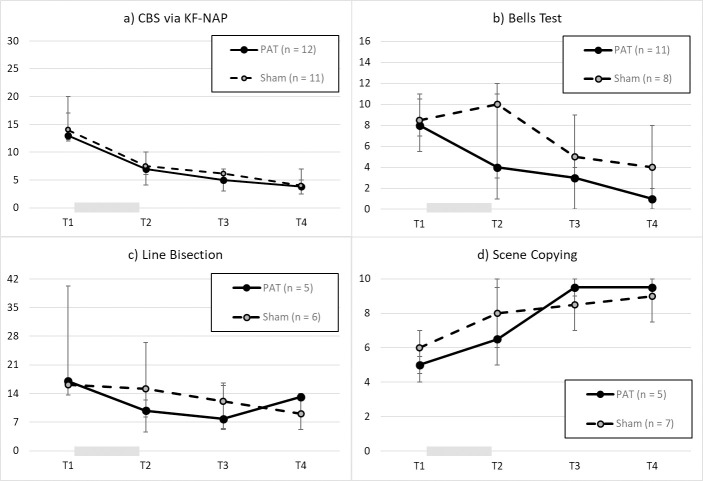
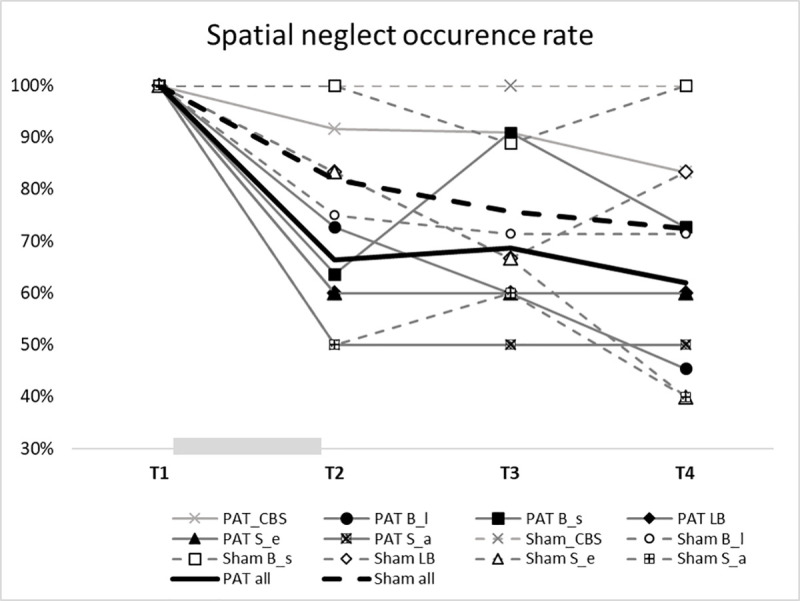
Spatial neglect (SN) is a common cognitive disorder after brain injury. Prism adaptation treatment (PAT) is one of the promising interventions for SN albeit inconsistent results from previous studies. We carried out a comparison intervention (PAT vs. Sham) and aimed to evaluate the efficacy of PAT on visuospatial symptoms of SN in an inpatient rehabilitation setting that offered a highly intensive comprehensive brain injury rehabilitation program. A total of 34 patients with moderate-to-severe SN secondary to stroke or traumatic brain injury were randomized to the PAT group and the Sham group (an active control group). Both groups received 10 sessions of treatment, over two weeks, in addition to the rehabilitation therapies provided by their rehabilitation care teams. Outcomes were measured using an ecological instrument (the Catherine Bergego Scale) and paper-and-pencil tests (the Bells Test, the Line Bisection Test and the Scene Copying Test). Patients were assessed at baseline, immediately after treatment, two weeks after treatment, and four weeks after treatment. 23 (67.6%) patients completed treatment and all the assessment sessions and were included in the final analyses using mixed linear modeling. While SN symptoms reduced in both groups, we found no difference between the two groups in the degree of improvement. In addition, the average SN recovery rates were 39.1% and 28.6% in the PAT and Sham groups, respectively, but this discrepancy did not reach statistical significance. Thus, the present study suggests that PAT may contribute little to SN care in the context of a highly intensive inpatient rehabilitation program. Further large-scale investigation is required to uncover the mechanisms underlying PAT and Sham in order to refine the treatment or create new interventions.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: Peii Chen is employed by Kessler Foundation, receiving funding from the State of New Jersey and the US federal government. Her work related to the present study is, however, not funded by external funding agency. Peii Chen is listed as the inventor on the US Patent (No. 10,739,618) related to the key element of the treatment equipment reported in the manuscript. Other authors have declared that no competing interests exist. Following patent was used in this study: Wearable System and Methods of Treatment of a Neurocognitive Condition (U.S. Patent Number 10,739,618). Patent owner: Kessler Foundation. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- Karnath H-O, Rorden C. The anatomy of spatial neglect. Neuropsychologia [Internet]. 2011/07/02. 2012. May;50(6):1010–7. Available from: https://pubmed.ncbi.nlm.nih.gov/21756924 10.1016/j.neuropsychologia.2011.06.027 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
