

Meningococcal carriage in periods of high and low invasive meningococcal disease incidence in the UK: comparison of UKMenCar1-4 cross-sectional survey results
- PMID: 33482143
- PMCID: PMC8064914
- DOI: 10.1016/S1473-3099(20)30842-2
Meningococcal carriage in periods of high and low invasive meningococcal disease incidence in the UK: comparison of UKMenCar1-4 cross-sectional survey results
Erratum in
-
Correction to Lancet Infect Dis 2021; 21: 677-87.Lancet Infect Dis. 2021 May;21(5):e122. doi: 10.1016/S1473-3099(21)00229-2. Lancet Infect Dis. 2021. PMID: 33894853 Free PMC article. No abstract available.
-
Correction to Lancet Infect Dis 2021; 21: 677-87.Lancet Infect Dis. 2021 Jul;21(7):e182. doi: 10.1016/S1473-3099(21)00266-8. Epub 2021 May 6. Lancet Infect Dis. 2021. PMID: 33965063 Free PMC article. No abstract available.
Abstract
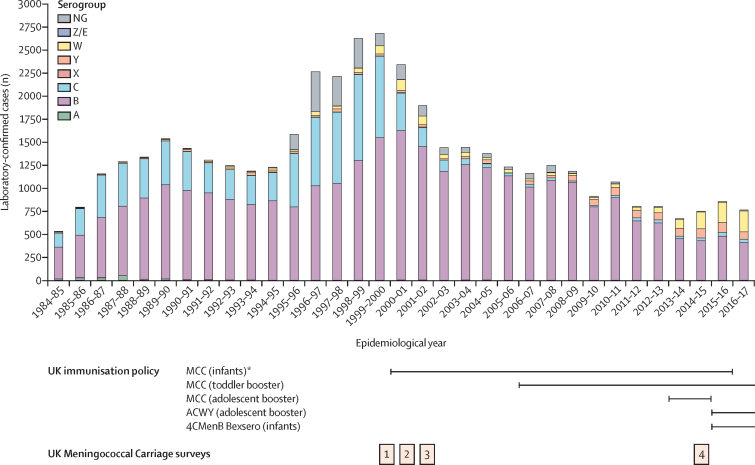
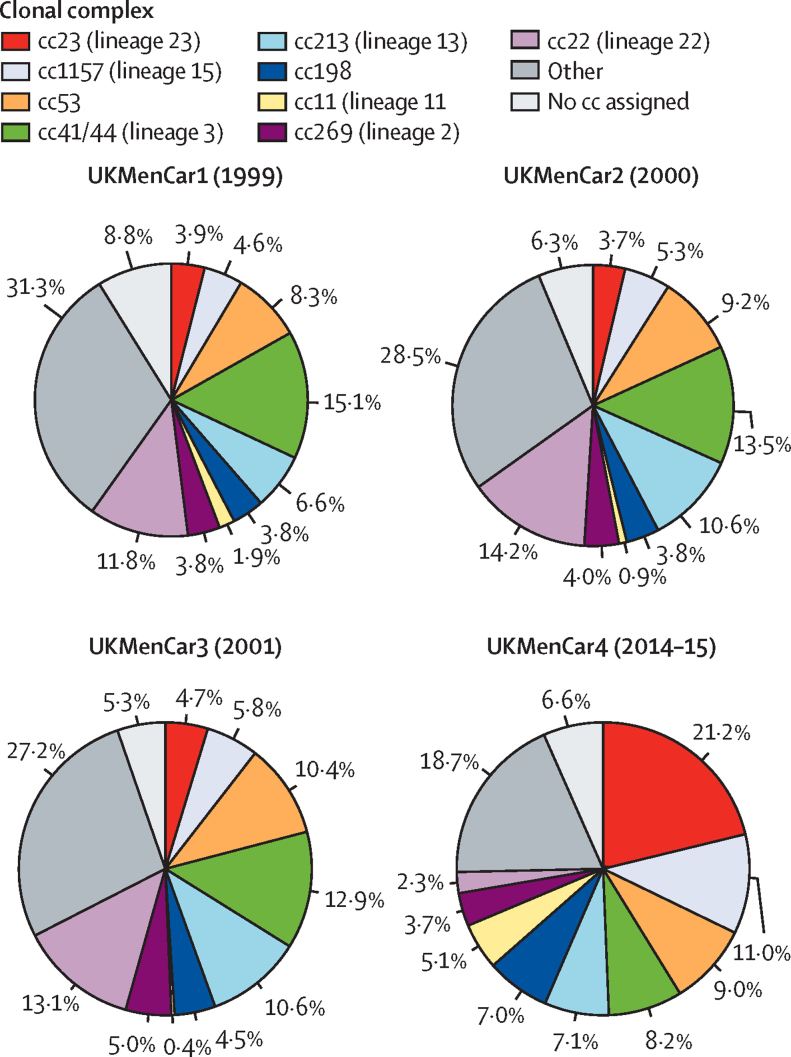
Background: The incidence of invasive meningococcal disease in the UK decreased by approximately four times from 1999 to 2014, with reductions in serogroup C and serogroup B disease. Lower serogroup C invasive meningococcal disease incidence was attributable to implementation of the meningococcal serogroup C conjugate vaccine in 1999, through direct and indirect protection, but no vaccine was implemented against serogroup B disease. UK Meningococcal Carriage surveys 1-3 (UKMenCar1-3), conducted in 1999, 2000, and 2001, were essential for understanding the impact of vaccination. To investigate the decline in invasive meningococcal disease incidence, we did a large oropharyngeal carriage survey in 2014-15, immediately before the changes to meningococcal vaccines in the UK national immunisation schedule.
Methods: UKMenCar4 was a cross-sectional survey in adolescents aged 15-19 years who were enrolled from schools and colleges geographically local to one of 11 UK sampling centres between Sept 1, 2014, and March 30, 2015. Participants provided an oropharyngeal swab sample and completed a questionnaire on risk factors for carriage, including social behaviours. Samples were cultured for putative Neisseria spp, which were characterised with serogrouping and whole-genome sequencing. Data from this study were compared with the results from the UKMenCar1-3 surveys (1999-2001).
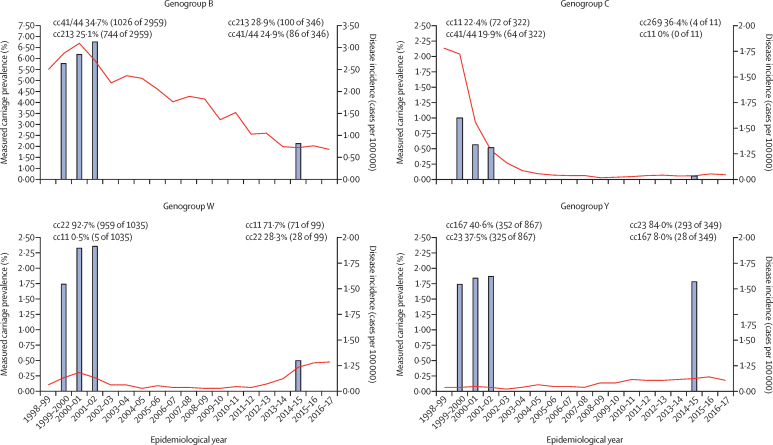
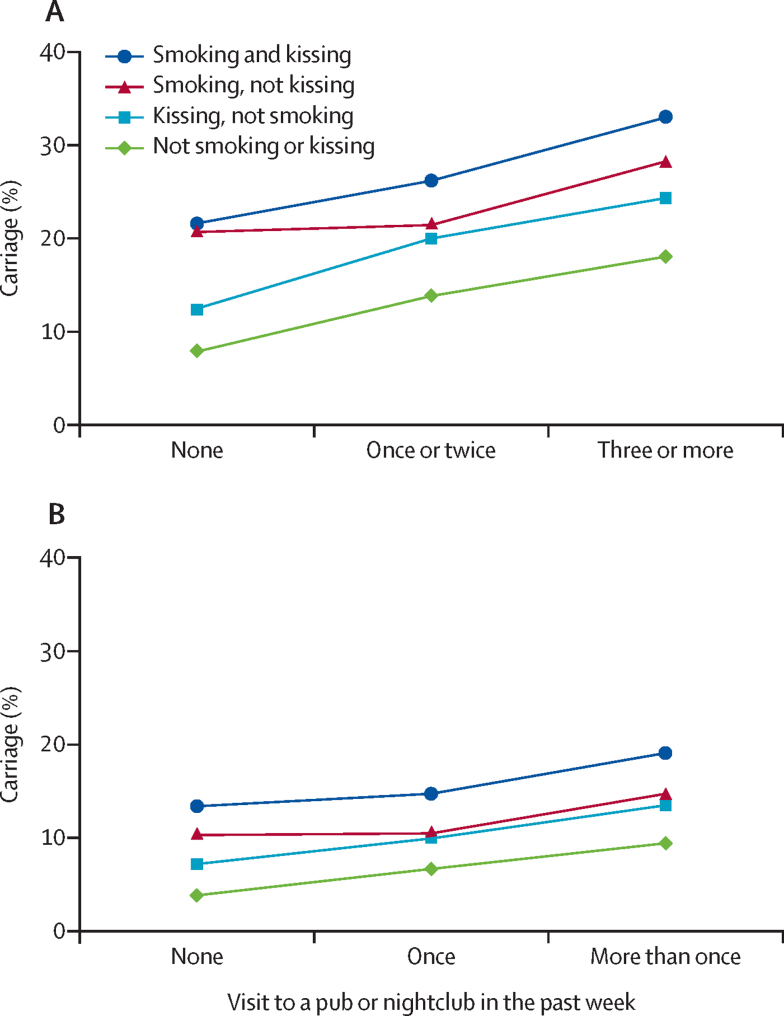
Findings: From the 19 641 participants (11 332 female, 8242 male, 67 not stated) in UKMenCar4 with culturable swabs and completed risk-factor questionnaires, 1420 meningococci were isolated, with a carriage prevalence of 7·23% (95% CI 6·88-7·60). Carriage prevalence was substantially lower in UKMenCar4 than in the previous surveys: carriage prevalence was 16·6% (95% CI 15·89-17·22; 2306/13 901) in UKMenCar1 (1999), 17·6% (17·05-18·22; 2873/16 295) in UKMenCar2 (2000), and 18·7% (18·12-19·27; 3283/17 569) in UKMenCar3 (2001). Carriage prevalence was lower for all serogroups in UKMenCar4 than in UKMenCar1-3, except for serogroup Y, which was unchanged. The prevalence of carriage-promoting social behaviours decreased from 1999 to 2014-15, with individuals reporting regular cigarette smoking decreasing from 2932 (21·5%) of 13 650 to 2202 (11·2%) of 19 641, kissing in the past week from 6127 (44·8%) of 13 679 to 7320 (37·3%) of 19 641, and attendance at pubs and nightclubs in the past week from 8436 (62·1%) of 13 594 to 7662 (39·0%) of 19 641 (all p<0·0001).
Interpretation: We show that meningococcal carriage prevalence in adolescents sampled nationally during a low incidence period (2014-15) was less than half of that in an equivalent population during a high incidence period (1999-2001). Disease and carriage caused by serogroup C was well controlled by ongoing vaccination. The prevalence of behaviours associated with carriage declined, suggesting that public health policies aimed at influencing behaviour might have further reduced disease.
Funding: Wellcome Trust, UK Department of Health, and National Institute for Health Research.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Stephens DS, Greenwood B, Brandtzaeg P. Epidemic meningitis, meningococcaemia, and Neisseria meningitidis. Lancet. 2007;369:2196–2210. - PubMed
-
- Christensen H, May M, Bowen L, Hickman M, Trotter CL. Meningococcal carriage by age: a systematic review and meta-analysis. Lancet Infect Dis. 2010;10:853–861. - PubMed
-
- Caugant DA. Genetics and evolution of Neisseria meningitidis: importance for the epidemiology of meningococcal disease. Infect Genet Evol. 2008;8:558–565. - PubMed
-
- Harrison LH, Trotter CL, Ramsay ME. Global epidemiology of meningococcal disease. Vaccine. 2009;27(suppl 2):B51–B63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
