

Risk factors and comorbidities associated with magnesium deficiency in pregnant women and women with hormone-related conditions: analysis of a large real-world dataset
- PMID: 33482760
- PMCID: PMC7821493
- DOI: 10.1186/s12884-021-03558-2
Risk factors and comorbidities associated with magnesium deficiency in pregnant women and women with hormone-related conditions: analysis of a large real-world dataset
Abstract
Background: An accumulating body of literature indicates that magnesium deficiency is associated with a number of hormone-related conditions (HRC) in women, and epidemiological studies are needed to assess its prevalence and risk factors. Here, we present a secondary analysis of data pooled from four large observational studies that assessed magnesium deficiency among pregnant women and women with HRC across the Russian Federation.
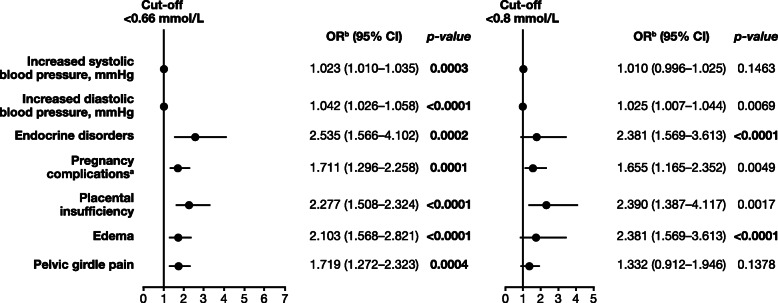
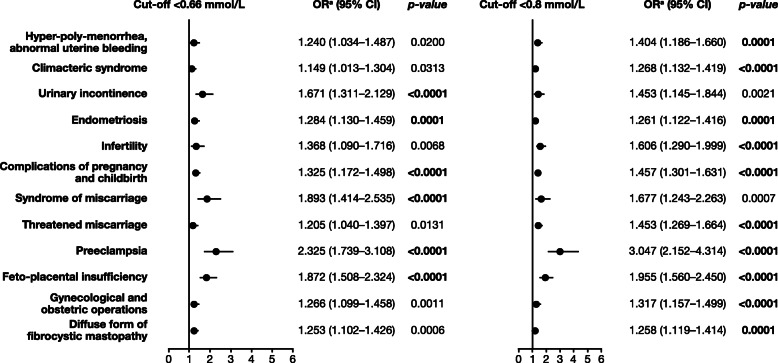
Methods: The main objective of this analysis was to estimate the prevalence of magnesium deficiency in this population and to describe risk factors and comorbidities associated with low serum magnesium. Univariate logistic regression analysis was performed to identify the risk factors and comorbid conditions associated with an increased risk of low serum magnesium level.
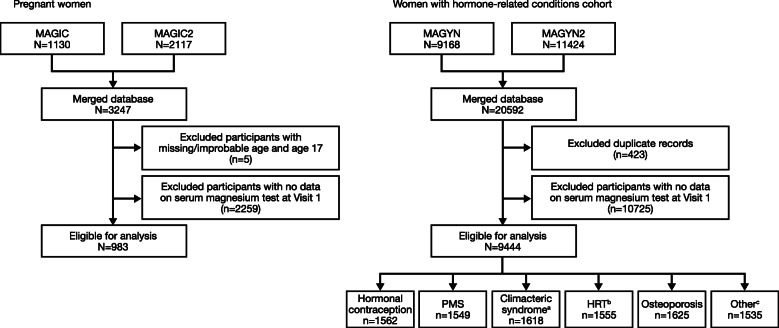
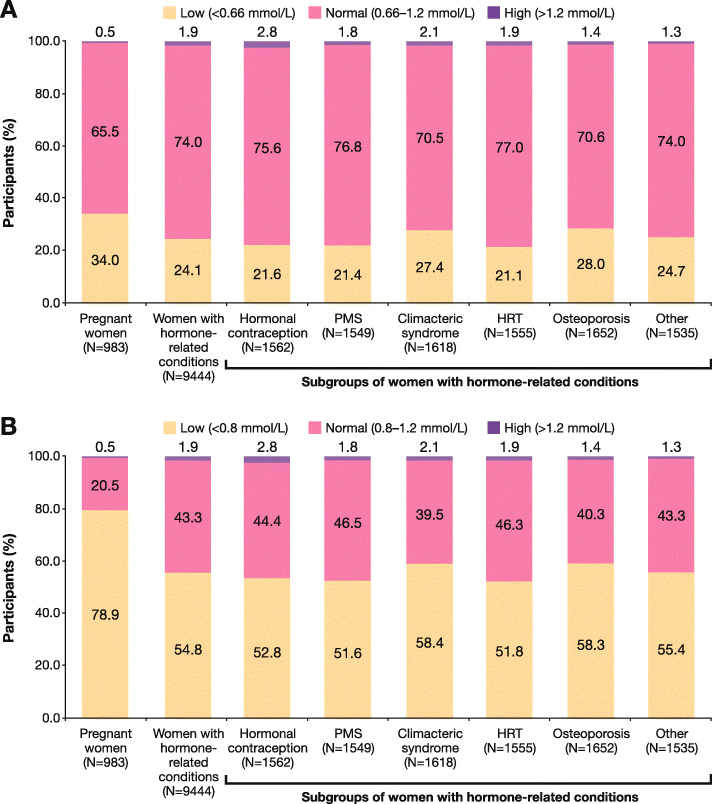
Results: A total of 983 pregnant women and 9444 women with HRC were eligible for analysis. Prevalence of hypomagnesemia (magnesium serum level cut-off < 0.66 mmol/L/< 0.8 mmol/L) was 34.0%/78.9% in pregnant women and 21.4%/54.8% in women with HRC. The highest prevalence of magnesium deficiency was observed for osteoporosis and climacteric syndrome. Risk factors included diastolic blood pressure, previous pregnancy complications, infections and edema for pregnant women, and age, body mass index, and various comorbidities for women with HRC.
Conclusions: These results confirm the high prevalence of hypomagnesemia in pregnant women and women with HRC and underline the importance of routine screening, since risk factors are mostly non-specific.
Keywords: Climacteric syndrome; Hormone replacement therapy; Magnesium deficiency; Oral contraceptives; Osteoporosis; Pregnancy.
Conflict of interest statement
Starostin K., Konchits S., and Bevz A are Sanofi employees. Other authors declare no potential conflict of interest.
Figures
Similar articles
-
Magnesium Deficiency Questionnaire: A New Non-Invasive Magnesium Deficiency Screening Tool Developed Using Real-World Data from Four Observational Studies.Nutrients. 2020 Jul 11;12(7):2062. doi: 10.3390/nu12072062. Nutrients. 2020. PMID: 32664490 Free PMC article.
-
The prevalence of serum magnesium and iron deficiency anaemia among Sudanese women in early pregnancy: a cross-sectional study.Trans R Soc Trop Med Hyg. 2019 Jan 1;113(1):31-35. doi: 10.1093/trstmh/try109. Trans R Soc Trop Med Hyg. 2019. PMID: 30325455
-
Maternal Vitamin D Status and Its Related Factors in Pregnant Women in Bangkok, Thailand.PLoS One. 2015 Jul 6;10(7):e0131126. doi: 10.1371/journal.pone.0131126. eCollection 2015. PLoS One. 2015. PMID: 26147381 Free PMC article.
-
Gitelman syndrome-associated severe hypokalemia and hypomagnesemia: case report and review of the literature.J Matern Fetal Neonatal Med. 2010 Nov;23(11):1301-4. doi: 10.3109/14767051003678010. J Matern Fetal Neonatal Med. 2010. PMID: 20350237 Review.
-
[Magnesium deficiency in an endocrinologist's practice].Klin Med (Mosk). 2008;86(7):47-51. Klin Med (Mosk). 2008. PMID: 18756748 Review. Russian.
Cited by
-
Influence of Isoflavones and Probiotics on Magnesium Status in Healthy Female Rats.Foods. 2023 Oct 25;12(21):3908. doi: 10.3390/foods12213908. Foods. 2023. PMID: 37959026 Free PMC article.
-
Magnesium deficiency and dilated cardiomyopathy diagnosed peripartum.Obstet Med. 2025 Jun 16:1753495X251349950. doi: 10.1177/1753495X251349950. Online ahead of print. Obstet Med. 2025. PMID: 40535201 Free PMC article. Review.
-
Magnesium level correlation with clinical status and quality of life in women with hormone related conditions and pregnancy based on real world data.Sci Rep. 2021 Mar 11;11(1):5734. doi: 10.1038/s41598-021-85156-y. Sci Rep. 2021. PMID: 33707700 Free PMC article.
-
Magnesium: Exploring Gender Differences in Its Health Impact and Dietary Intake.Nutrients. 2025 Jul 4;17(13):2226. doi: 10.3390/nu17132226. Nutrients. 2025. PMID: 40647330 Free PMC article. Review.
-
Cardiometabolic Risk Factors Associated with Magnesium and Vitamin D Nutrients during Pregnancy-A Narrative Review.Nutrients. 2024 Aug 9;16(16):2630. doi: 10.3390/nu16162630. Nutrients. 2024. PMID: 39203767 Free PMC article. Review.
References
-
- Ismail AAA, Ismail NA. Magnesium: A mineral essential for health yet generally underestimated or even ignored. J Nutr Food Sci. 2016;6:523. 10.4172/2155-9600.1000523.
-
- Costello RB, Elin RJ, Rosanoff A, Wallace TC, Guerrero-Romero F, Hruby A, Lutsey PL, Nielsen FH, Rodriguez-Moran M, Song Y, et al. Perspective: the case for an evidence-based reference interval for serum magnesium: the time has come. Adv Nutr. 2016;7(6):977–993. doi: 10.3945/an.116.012765. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
