

Clinico-pathologic determinants of non-e-curative outcome following en-bloc endoscopic submucosal dissection in patients with early gastric neoplasia
- PMID: 33482761
- PMCID: PMC7824923
- DOI: 10.1186/s12885-020-07762-9
Clinico-pathologic determinants of non-e-curative outcome following en-bloc endoscopic submucosal dissection in patients with early gastric neoplasia
Abstract
Background: Endoscopic submucosal dissection (ESD) is gaining enormous popularity in the treatment of early gastric cancers (EGCs) in many institutions across the world. However, appropriate selection of candidates for endoscopic resection is crucial to sufficiently mitigate non-e-curative (NEC) resection. This study aims at identifying the various clinico-pathologic factors that independently predict the NEC outcome and depth of submucosal invasion following ESD procedure in patients with EGC.
Methods: Multiple logistic regression analysis was applied to investigate factors that independently predict both non-curability phenomenon and the level of submucosal invasion in patients with early gastric neoplasia. Statistical Packages for the Social Sciences version 23 was used for analysis.
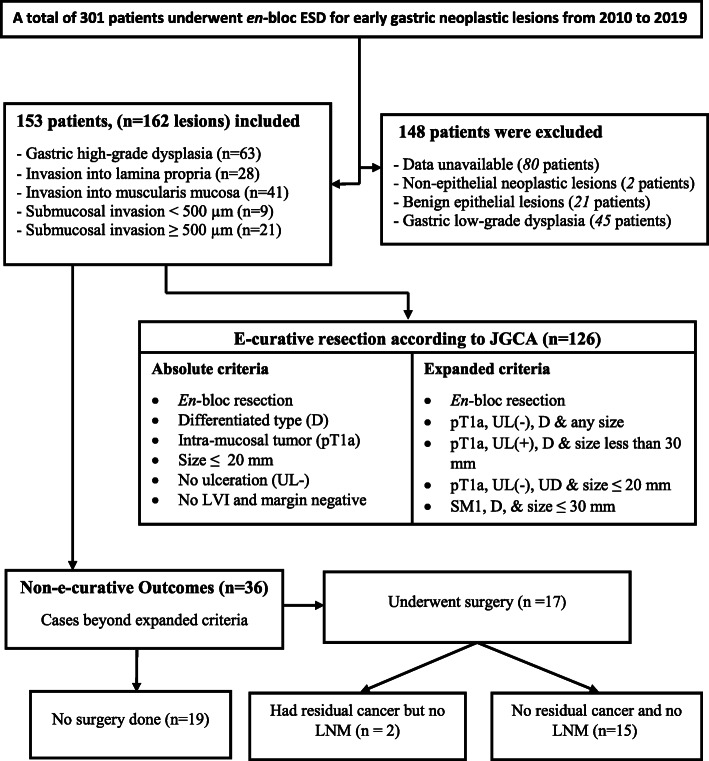
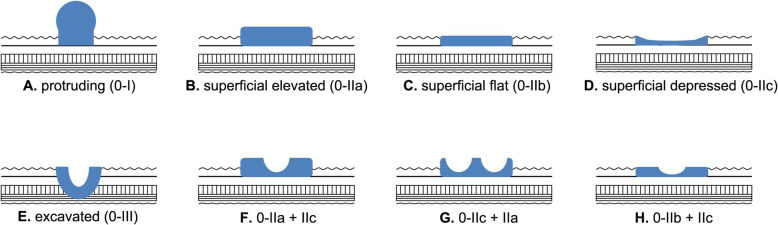
Results: A total of 153 patients (162 EGC lesions) underwent en-bloc ESD after which the rate of complete resection and non-e-curative outcome were 95% and 22.2%, correspondingly. Multivariate analysis depicted that tumor location in the upper two third of stomach (odds ratio [OR], 5.46; 95% confidence interval [95% CI], 1.65-18.12; p = 0.006), tumor size > 2 cm (OR, 7.63; 95% CI, 2.29-25.42; p = 0.001), histologically undifferentiated tumor (OR, 15.54; 95% CI, 1.65-146.22; p = 0.001), and tumors with 0-IIa/0-IIc or their mixed variants with predominant 0-IIa/0-IIc (OR, 9.77; 95% CI, 1.23-77.65; p = 0.031) were all independent predictors of NEC resection for early gastric tumors. Additionally, location in the upper two third of the stomach (OR, 8.88; 95% CI, 2.90-27.17; p < 0.001), ulcerated lesions (OR, 3.70; 95% CI, 1.15-11.90; p = 0.028), lesions with > 2 cm (OR, 2.94; 95% CI, 1.08-8.02; p = 0.036) and those with poor differentiation (OR, 6.51; 95% CI, 2.23-18.98; p = 0.001) were found to have significant association with submucosal invasion.
Conclusions: Tumors located in the upper two third of the stomach having a larger size (> 2 cm), poor histo-differentiation and a gross type of 0-IIa/0-IIc or their mixed variants with predominant 0-IIa/0-IIc were significantly associated with a risk of NEC after ESD procedure. Thus, early gastric tumors displaying these features need to be handled carefully during endoscopic resection. Our findings may shed light on the pre-procedural detection of clinicopathologic factors that determine non-e-curability in patients with EGC.
Keywords: Clinico-pathologic factors; ESD; Early gastric cancer; Non-e-curative resection.
Conflict of interest statement
The authors declare that they have no conflicts of interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
