

Cost of hospital care of women with postpartum haemorrhage in India, Kenya, Nigeria and Uganda: a financial case for improved prevention
- PMID: 33482858
- PMCID: PMC7821537
- DOI: 10.1186/s12978-020-01063-x
Cost of hospital care of women with postpartum haemorrhage in India, Kenya, Nigeria and Uganda: a financial case for improved prevention
Erratum in
-
Correction to: Cost of hospital care of women with postpartum haemorrhage in India, Kenya, Nigeria and Uganda: a financial case for improved prevention.Reprod Health. 2021 Mar 6;18(1):57. doi: 10.1186/s12978-021-01110-1. Reprod Health. 2021. PMID: 33676501 Free PMC article. No abstract available.
Abstract
Objective: Access to quality, effective lifesaving uterotonics in low and middle-income countries (LMICs) remains a major barrier to reducing maternal deaths from postpartum haemorrhage (PPH). Our objective was to assess the costs of care for women who receive different preventative uterotonics, and with PPH and no-PPH so that the differences, if significant, can inform better resource allocation for maternal health care.
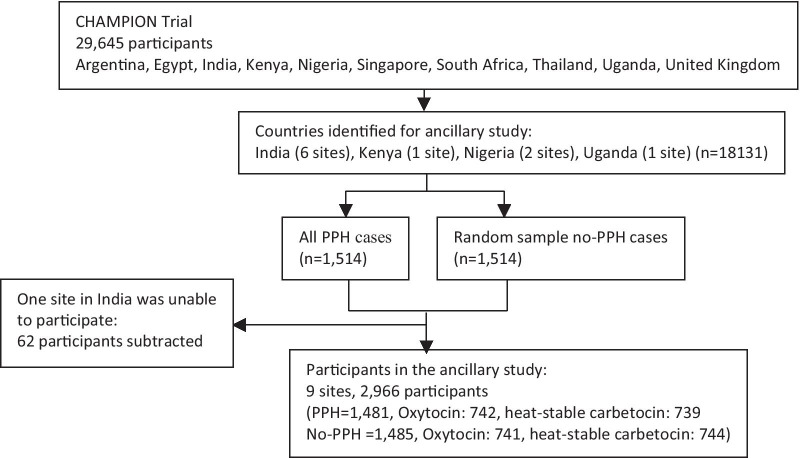
Methods: The costs of direct hospital care of women who received oxytocin or heat-stable carbetocin for prevention of PPH in selected tertiary care facilities in India, Kenya, Nigeria, and Uganda were assessed. We collected data from all women who had PPH, as well as a random sample of women without PPH. Cost data was collected for the cost of stay, PPH interventions, transfusions and medications for 2966 women. We analyzed the difference in cost of care at a facility level between women who experienced a PPH event and those who did not. Key findings The mean cost of care of a woman experiencing PPH in the study sites in India, Kenya, Nigeria, and Uganda exceeded the cost of care of a woman who did not experience PPH by between 21% and 309%. There was a large variation in cost across hospitals within a country and across countries.
Conclusion: Our results quantify the increased cost of PPH of up to 4.1 times that for a birth without PPH. PPH cost information can help countries to evaluate options across different conditions and in the formulation of appropriate guidelines for intrapartum care, including rational selection of quality-assured, effective medicines. This information can be applied to national assessment and adaptation of international recommendations such as the World Health Organization's recommendations on uterotonics for the prevention of PPH or other interventions used to treat PPH. Trial registration HRP Trial A65870; UTN U1111-1162-8519; ACTRN12614000870651; CTRI/2016/05/006969, EUDRACT 2014-004445-26. Date of registration 14 August 2014 Access to quality, effective lifesaving medicines in low and middle-income countries remains a major barrier to reducing maternal deaths from bleeding after childbirth. Information on to what extent treatments for bleeding increases the cost of care of women after childbirth is important for informed resource allocation. We collected data from all women who had bleeding after childbirth, as well as a random sample of women without bleeding in selected hospitals in India, Kenya, Nigeria, and Uganda. Cost data was collected for the cost of stay and interventions to manage bleeding for 2966 women. We compared the difference in cost of care between women who experienced a bleeding event and those who did not. The mean cost of care of a woman with bleeding in the study sites exceeded the cost of care of a woman who did not experience PPH by between 21% and 309%. There was a large variation in cost across hospitals within a country and across countries. Our results indicate an increased cost of bleeding of up to 4.1 times that for birth without bleeding. Effective prevention reduces the cost of care. Cost information can help countries to evaluate options across different conditions and in the formulation of appropriate guidelines for intrapartum care, including rational selection of quality-assured, effective medicines. This information can be applied to national assessment and adaptation of international recommendations such as the World Health Organization's recommendations on medications for the prevention of bleeding after childbirth or other interventions used to treat bleeding.
Keywords: Cost; Heat stable carbetocin; Oxytocin; PPH; Postpartum haemorrhage.
Conflict of interest statement
We declare no competing interests.
References
-
- WHO. Maternal Mortality Factsheet. World Health Organization. 2018. https://www.who.int/news-room/fact-sheets/detail/maternal-mortality.
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
