

Cardiotoxic Potential of Hydroxychloroquine, Chloroquine and Azithromycin in Adult Human Primary Cardiomyocytes
- PMID: 33483756
- PMCID: PMC7928616
- DOI: 10.1093/toxsci/kfaa194
Cardiotoxic Potential of Hydroxychloroquine, Chloroquine and Azithromycin in Adult Human Primary Cardiomyocytes
Abstract
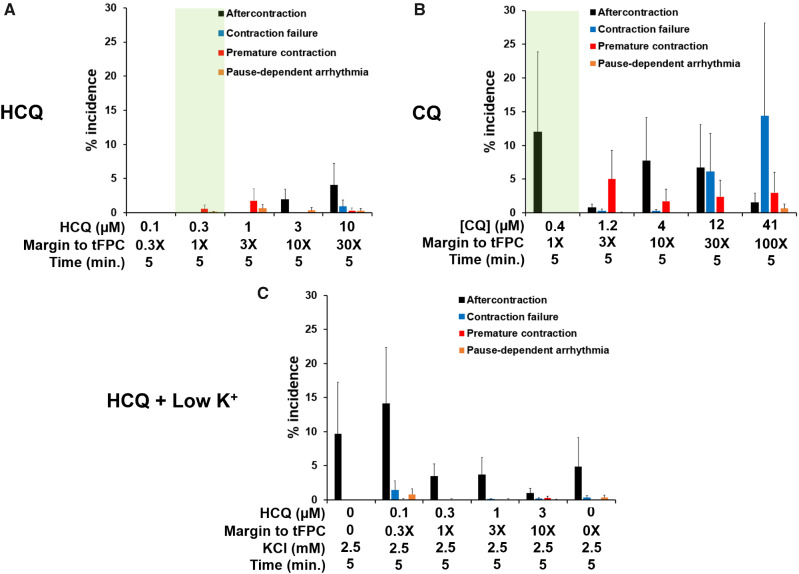
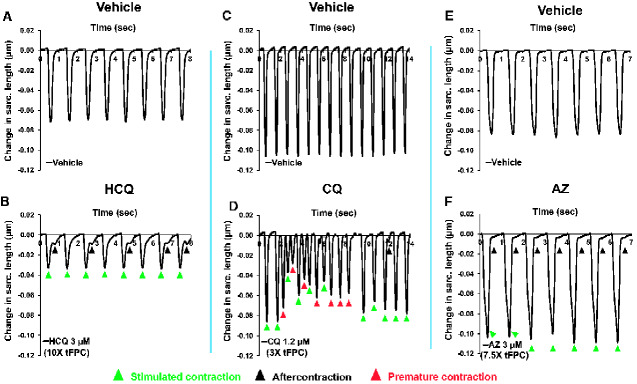
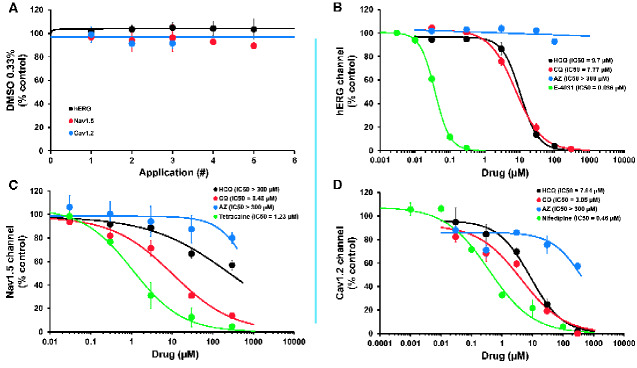
Substantial efforts have been recently committed to develop coronavirus disease-2019 (COVID-19) medications, and Hydroxychloroquine alone or in combination with Azithromycin has been promoted as a repurposed treatment. Although these drugs may increase cardiac toxicity risk, cardiomyocyte mechanisms underlying this risk remain poorly understood in humans. Therefore, we evaluated the proarrhythmia risk and inotropic effects of these drugs in the cardiomyocyte contractility-based model of the human heart. We found Hydroxychloroquine to have a low proarrhythmia risk, whereas Chloroquine and Azithromycin were associated with high risk. Hydroxychloroquine proarrhythmia risk changed to high with low level of K+, whereas high level of Mg2+ protected against proarrhythmic effect of high Hydroxychloroquine concentrations. Moreover, therapeutic concentration of Hydroxychloroquine caused no enhancement of elevated temperature-induced proarrhythmia. Polytherapy of Hydroxychloroquine plus Azithromycin and sequential application of these drugs were also found to influence proarrhythmia risk categorization. Hydroxychloroquine proarrhythmia risk changed to high when combined with Azithromycin at therapeutic concentration. However, Hydroxychloroquine at therapeutic concentration impacted the cardiac safety profile of Azithromycin and its proarrhythmia risk only at concentrations above therapeutic level. We also report that Hydroxychloroquine and Chloroquine, but not Azithromycin, decreased contractility while exhibiting multi-ion channel block features, and Hydroxychloroquine's contractility effect was abolished by Azithromycin. Thus, this study has the potential to inform clinical studies evaluating repurposed therapies, including those in the COVID-19 context. Additionally, it demonstrates the translational value of the human cardiomyocyte contractility-based model as a key early discovery path to inform decisions on novel therapies for COVID-19, malaria, and inflammatory diseases.
Keywords: COVID-19; adult human primary cardiomyocyte; contractility; hydroxychloroquine; proarrhythmia risk; translation.
© The Author(s) 2021. Published by Oxford University Press on behalf of the Society of Toxicology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures


References
-
- Abi-Gerges N., Miller P. E., Ghetti A. (2020a). Human heart cardiomyocytes in drug discovery and research: New opportunities in translational sciences. Curr. Pharm. Biotechnol. 21, 787–806. - PubMed
-
- Arellano-Rodrigo E., García A., Mont L., Roqué M. (2001). Torsade de pointes and cardiorespiratory arrest induced by azithromycin in a patient with congenital long QT syndrome. Med. Clin. (Barc) 117, 118–119. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
