

Neuropathologic findings of patients with COVID-19: a systematic review
- PMID: 33483885
- PMCID: PMC7822400
- DOI: 10.1007/s10072-021-05068-7
Neuropathologic findings of patients with COVID-19: a systematic review
Abstract
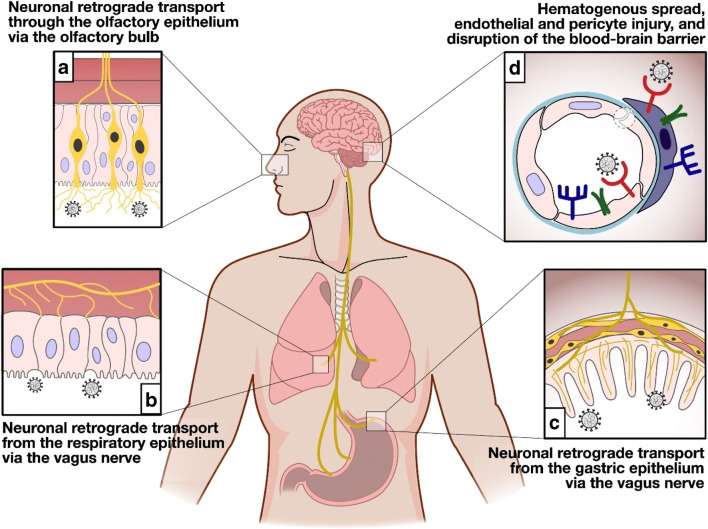
Background: Despite the expanding literature that discusses insights into the clinical picture and mechanisms by which the SARS-CoV-2 virus invades the nervous system, data on the neuropathologic findings of patients who died following SARS-CoV-2 infection is limited.
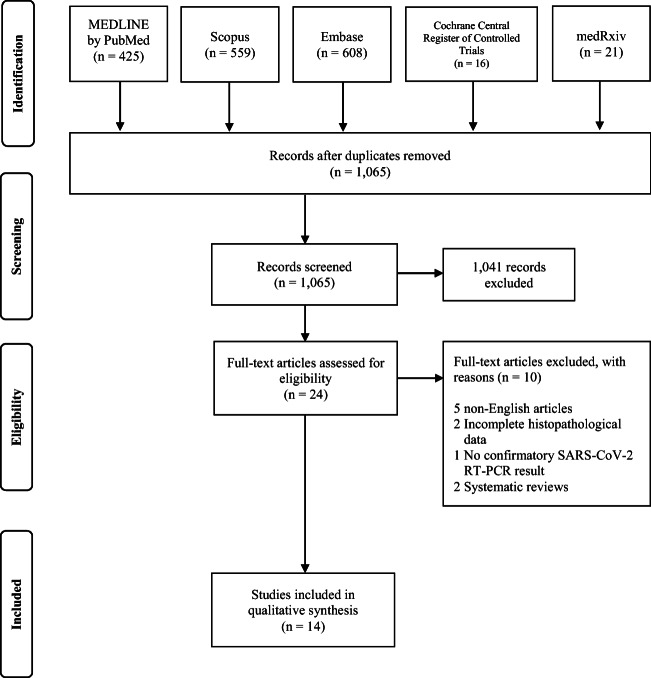
Methods: A broad literature search was done for published articles that reported on histopathological findings of the brain in patients with COVID-19 in PubMed by MEDLINE, Embase, CENTRAL by the Cochrane Library, and SCOPUS from December 31, 2019 to October 31, 2020.
Results: The systematic literature search strategy used resulted in a total of 1608 articles of which 14 were included in the analysis (PROSPERO registration number: CRD42020221022). There were ten case series, two case reports, one retrospective cohort, and one prospective cohort. The age of the patients ranged between 38 and 90 years old, most of them older than 65 years old (n=66, 45.2%) and males (n=79, 54.1%). Most tested negative in SARS-CoV-2 immunohistochemistry (n=70, 47.9%). The striking pathologic changes included diffuse edema (n=25, 17.1%), gliosis with diffuse activation of microglia and astrocytes (n=52, 35.6%), infarctions involving cortical and subcortical areas of the brain (n=4, 2.7%), intracranial bleed (subarachnoid hemorrhage and punctate hemorrhages) (n=18, 12.4%), arteriosclerosis (n=43, 29.5%), hypoxic-ischemic injury (n=41, 28.1%), and signs of inflammation (n=52, 35.6%). The cause of death was attributed to the cardiorespiratory system (n=66, 45.2%).
Conclusions: The neuropathologic changes observed likely represent direct cytopathic effects and indirect effects secondary to host-specific inflammatory response induced by the viral infection. Further studies however are required to better elucidate the pathologic mechanism.
Keywords: COVID-19; Neuropathology; SARS-CoV-2.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Tsivgoulis G, Palaiodimou L, Katsanos AH, Caso V, Köhrmann M, Molina C, Cordonnier C, Fischer U, Kelly P, Sharma VK, Chan AC, Zand R, Sarraj A, Schellinger PD, Voumvourakis KI, Grigoriadis N, Alexandrov AV, Tsiodras S. Neurological manifestations and implications of COVID-19 pandemic. Ther Adv Neurol Disord. 2020;13:175628642093203. doi: 10.1177/1756286420932036. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
