

Targeting Insulin Resistance to Treat Cognitive Dysfunction
- PMID: 33483903
- PMCID: PMC9196144
- DOI: 10.1007/s12035-021-02283-3
Targeting Insulin Resistance to Treat Cognitive Dysfunction
Abstract
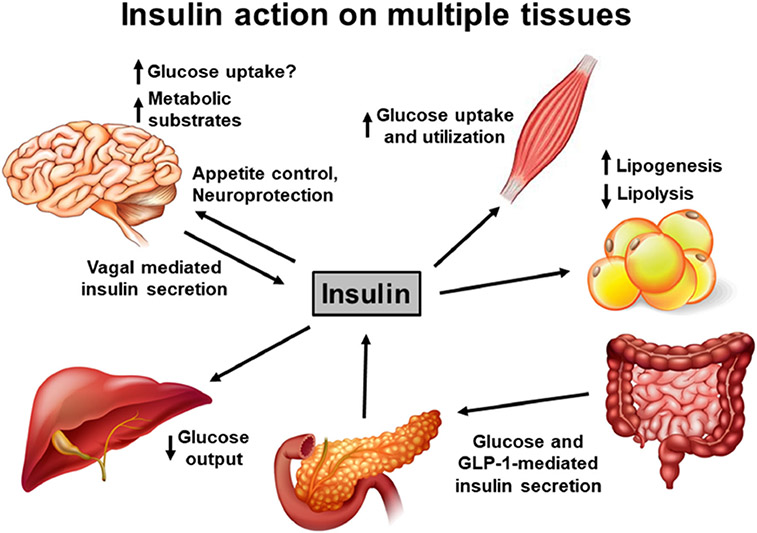
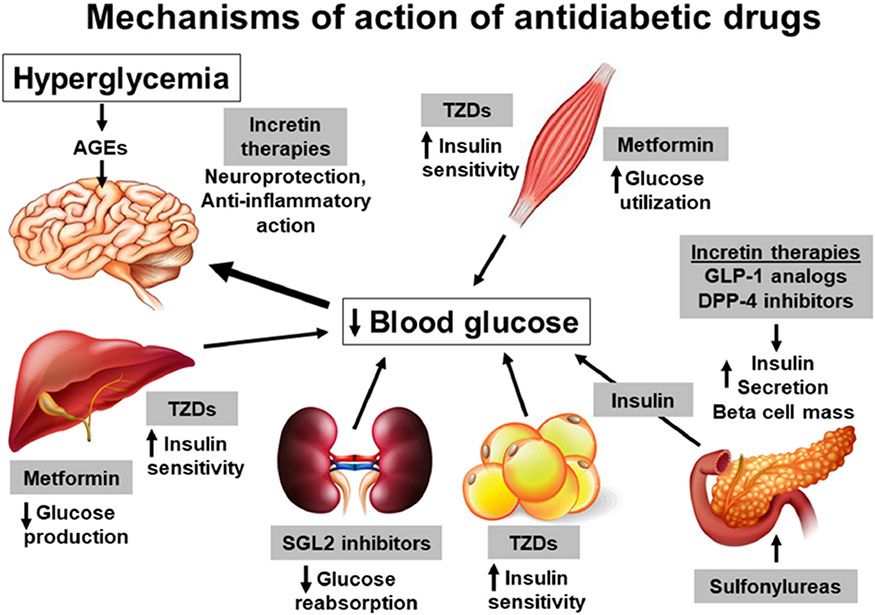
Dementia is a devastating disease associated with aging. Alzheimer's disease is the most common form of dementia, followed by vascular dementia. In addition to clinically diagnosed dementia, cognitive dysfunction has been reported in diabetic patients. Recent studies are now beginning to recognize type 2 diabetes mellitus, characterized by chronic hyperglycemia and insulin resistance, as a risk factor for Alzheimer's disease and other cognitive disorders. While studies on insulin action have remained traditionally in the domain of peripheral tissues, the detrimental effects of insulin resistance in the central nervous system on cognitive dysfunction are increasingly being reported by recent clinical and preclinical studies. The findings from these studies suggest that antidiabetic drugs have the potential to be used to treat dementia. In this review, we discuss the physiological functions of insulin in the brain, studies on the evaluation of cognitive function under conditions of insulin resistance, and reports on the beneficial actions of antidiabetic drugs in the brain. This review covers clinical studies as well as investigations in animal models and will further highlight the emerging link between insulin resistance and neurodegenerative disorders.
Keywords: Alzheimer’s disease; Dementia; Diabetes; Insulin resistance; Metabolic syndrome; Obesity.
Conflict of interest statement
Figures
References
-
- Hersom M, Helms HC, Schmalz C, Pedersen TA, Buckley ST, Brodin B (2018) The insulin receptor is expressed and functional in cultured blood-brain barrier endothelial cells but does not mediate insulin entry from blood to brain. Am J Physiol Endocrinol Metab 315(4):E531–E542. 10.1152/ajpendo.00350.2016 - DOI - PubMed
-
- Konishi M, Sakaguchi M, Lockhart SM, Cai W, Li ME, Homan EP, Rask-Madsen C, Kahn CR (2017) Endothelial insulin receptors differentially control insulin signaling kinetics in peripheral tissues and brain of mice. Proc Natl Acad Sci U S A 114(40): E8478–E8487. 10.1073/pnas.1710625114 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
