

Real world outcomes of combination and timing of immunotherapy with radiotherapy for melanoma with brain metastases
- PMID: 33484100
- PMCID: PMC7926022
- DOI: 10.1002/cam4.3716
Real world outcomes of combination and timing of immunotherapy with radiotherapy for melanoma with brain metastases
Abstract
Introduction: Immunotherapy (IT) and radiotherapy (RT) have improved overall survival in patients with melanoma with brain metastasis (MBM). We examined the real-world survival impact of IT and RT combination and timing strategies.
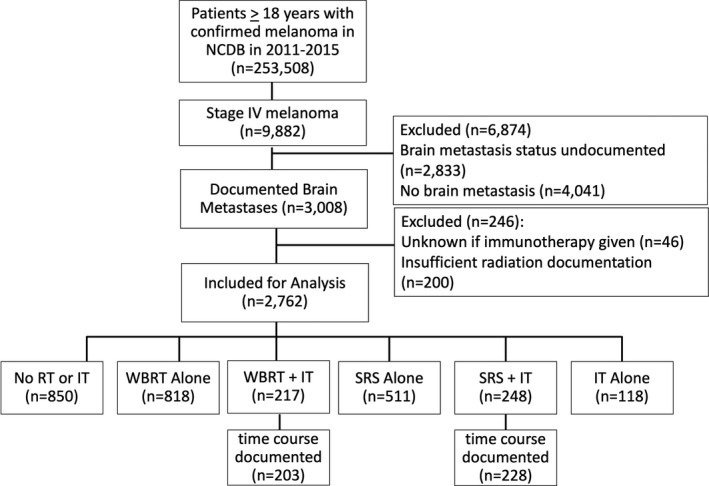
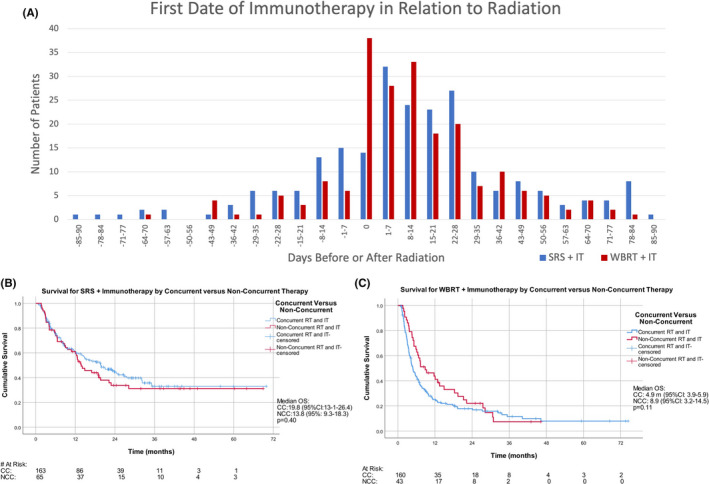
Materials and methods: From the facility-based National Cancer Database (NCDB) data set, 3008 cases of MBM were identified between 2011 and 2015. Six treatment cohorts were identified: stereotactic radiosurgery (SRS) + IT, SRS alone, whole brain radiotherapy (WBRT) + IT, WBRT alone, IT alone, and none. Concurrent therapy was defined as IT given within 28 days before or after RT; nonconcurrent defined as IT administered within 28-90 days of RT. The co-primary outcomes were propensity score-adjusted overall survival by treatment regimen and overall survival by RT and IT timing.
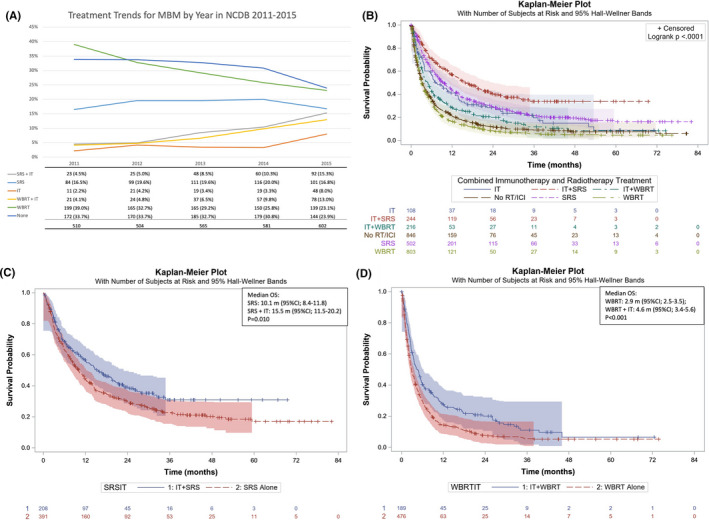
Results: Median overall survival (mOS) was performed for each treatment category; SRS +IT 15.77 m; (95%CI 12.13-21.29), SRS alone (9.33 m; 95%CI: 8.0-11.3), IT alone (7.29 m; 95%CI: 5.35-12.91), WBRT +IT (4.89 m; 95%CI: 3.65-5.92), No RT or IT (3.29 m; 95%CI: 2.96-3.75), and WBRT alone (3.12 m; 95%CI 2.79-3.52). By propensity score matching, mOS for SRS +IT (15.5 m; 95%CI: 11.5-20.2) was greater than SRS alone (10.1 m; 95%CI: 8.4-11.8) (p = 0.010), and median survival for WBRT +IT (4.6 m; 95%CI: 3.4-5.6) was greater than WBRT alone (2.9 m; 95%CI: 2.5-3.5) (p < 0.001). In the SRS +IT group, 24-month landmark survival was 47% (95%CI; 42-52) for concurrent versus 37% (95%CI; 30-44) for nonconcurrent (p = 0.40).
Conclusion: Those who received IT in addition to WBRT and SRS experienced longer survival compared to RT modalities alone, while those receiving concurrent SRS and IT trended toward improved survival versus nonconcurrent therapy.
Keywords: NCDB; brain metastasis; immunotherapy; melanoma; stereotactic radiosurgery; whole brain radiotherapy.
© 2021 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
JTM received travel compensation from Astellas pharmaceuticals. ECG, JP, DS, DS, and GN report no conflicts of interest.
Figures
Similar articles
-
Stereotactic radiosurgery and immunotherapy in melanoma brain metastases: Patterns of care and treatment outcomes.Radiother Oncol. 2018 Aug;128(2):266-273. doi: 10.1016/j.radonc.2018.06.017. Epub 2018 Jun 27. Radiother Oncol. 2018. PMID: 29960685
-
Impact of radiation, systemic therapy and treatment sequencing on survival of patients with melanoma brain metastases.Eur J Cancer. 2019 Mar;110:11-20. doi: 10.1016/j.ejca.2018.12.023. Epub 2019 Feb 7. Eur J Cancer. 2019. PMID: 30739835
-
Melanoma brain metastases: is it time to eliminate radiotherapy?J Neurooncol. 2020 Aug;149(1):27-33. doi: 10.1007/s11060-020-03485-w. Epub 2020 Jun 15. J Neurooncol. 2020. PMID: 32556863
-
The treatment of brain metastases from malignant melanoma.Semin Oncol. 2002 Oct;29(5):518-24. doi: 10.1053/sonc.2002.35247. Semin Oncol. 2002. PMID: 12407517 Review.
-
Treatment of melanoma brain metastases with radiation and immunotherapy or targeted therapy: A systematic review with meta-analysis.Crit Rev Oncol Hematol. 2024 Oct;202:104462. doi: 10.1016/j.critrevonc.2024.104462. Epub 2024 Aug 2. Crit Rev Oncol Hematol. 2024. PMID: 39097248
Cited by
-
Immunotherapy and Modern Radiotherapy Technique for Older Patients with Locally Advanced Head and Neck Cancer: A Proposed Paradigm by the International Geriatric Radiotherapy Group.Cancers (Basel). 2022 Oct 27;14(21):5285. doi: 10.3390/cancers14215285. Cancers (Basel). 2022. PMID: 36358703 Free PMC article.
-
The cure from within? a review of the microbiome and diet in melanoma.Cancer Metastasis Rev. 2022 Jun;41(2):261-280. doi: 10.1007/s10555-022-10029-3. Epub 2022 Apr 27. Cancer Metastasis Rev. 2022. PMID: 35474500 Free PMC article. Review.
-
Progress in immunotherapy for brain metastatic melanoma.Front Oncol. 2025 Jan 28;14:1485532. doi: 10.3389/fonc.2024.1485532. eCollection 2024. Front Oncol. 2025. PMID: 39935851 Free PMC article. Review.
-
Melanoma Brain Metastases: A Retrospective Analysis of Prognostic Factors and Efficacy of Multimodal Therapies.Cancers (Basel). 2023 Feb 28;15(5):1542. doi: 10.3390/cancers15051542. Cancers (Basel). 2023. PMID: 36900333 Free PMC article.
-
Stereotactic radiosurgery for melanoma brain metastases: Concurrent immune checkpoint inhibitor therapy associated with superior clinicoradiological response outcomes.J Med Imaging Radiat Oncol. 2022 Jun;66(4):536-545. doi: 10.1111/1754-9485.13403. Epub 2022 Mar 27. J Med Imaging Radiat Oncol. 2022. PMID: 35343063 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394‐424. - PubMed
-
- Rastrelli M, Tropea S, Rossi CR, et al. Melanoma: epidemiology, risk factors, pathogenesis, diagnosis and classification. In Vivo. 2014;28:1005‐1011. - PubMed
-
- Davies MA, Liu P, McIntyre S, et al. Prognostic factors for survival in melanoma patients with brain metastases. Cancer. 2011;117:1687‐1696. - PubMed
-
- Patel JK, Didolkar MS, Pickren JW, et al. Metastatic pattern of malignant melanoma. A study of 216 autopsy cases. Am J Surg. 1978;135:807‐810. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
