

The Healthcare Cost Burden in Adults with High Risk for Cardiovascular Disease
- PMID: 33484443
- PMCID: PMC8333236
- DOI: 10.1007/s41669-021-00257-8
The Healthcare Cost Burden in Adults with High Risk for Cardiovascular Disease
Abstract
Objective: We calculated the short- and long-term care resource use and costs in adults with high-risk conditions for cardiovascular disease (HRCVD) as defined by the Canadian Cardiovascular Society dyslipidemia guidelines.
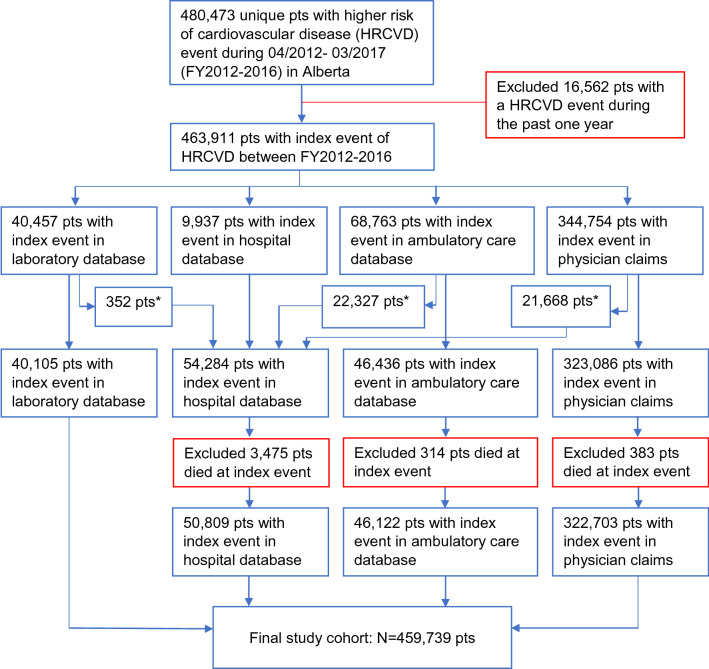
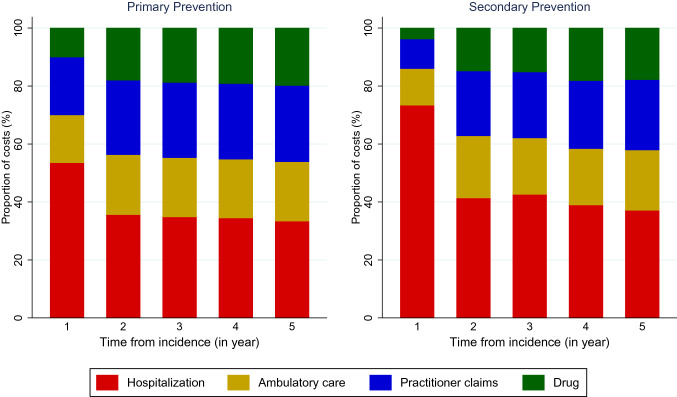
Methods: We linked Alberta health databases to identify patients aged ≥ 18 years with HRCVD between fiscal year (FY) 2012 and FY2016. The first HRCVD event was the index event. Patients were categorized into (1) primary prevention patients and (2) secondary prevention patients at the index event and were followed until death, they moved out of the province, or they were censored at March 2018. We calculated the resource use and costs for each of the 5 years after the index event.
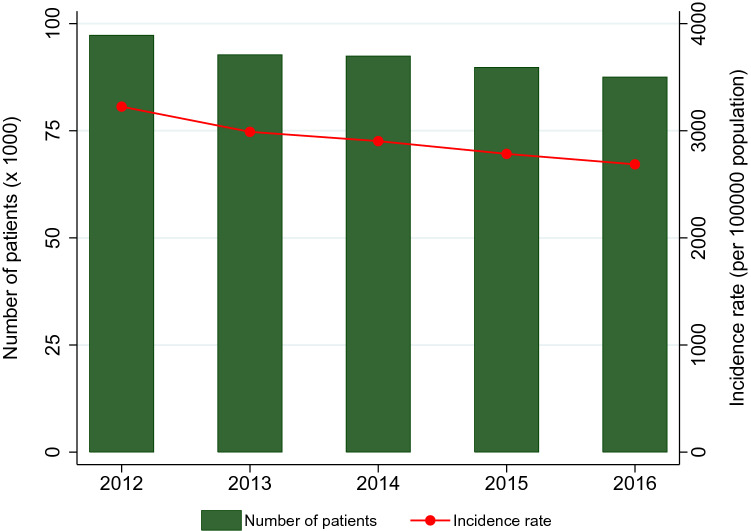
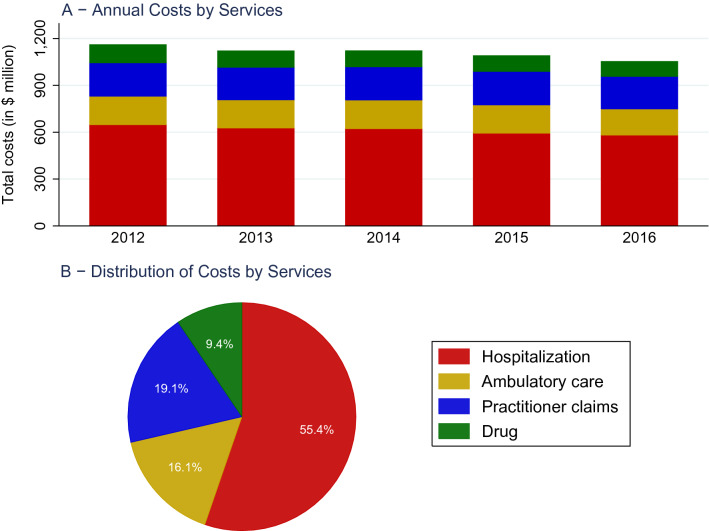
Results: The study included 459,739 HRCVD patients (13,947 [3%] were secondary prevention patients). The secondary prevention patients were older (median age 61 years vs. 55 years; p < 0.001), and there were fewer females in this group (30.4% vs. 51.3%; p < 0.001). The total healthcare costs in the first year decreased over time (FY2012: 1.16 billion Canadian dollars (CA$); FY2016: CA$1.05 billion; p < 0.001). An HRCVD patient incurred CA$12,068, CA$5626, and CA$4655 during the first, second, and fifth year, respectively (p for trend < 0.001). During the first year, healthcare costs per secondary prevention patient (CA$36,641) were triple that for a primary prevention patient (CA$11,299; p < 0.001), primarily due to higher hospitalization costs in secondary prevention patients (CA$26,896 vs. CA$6051; p < 0.001).
Conclusions: The healthcare costs for HRCVD patients were substantial but decreased over time. The costs were highest in the year following the index event and decreased thereafter. Secondary prevention patients incurred higher costs than the primary prevention patients.
© 2021. The Author(s).
Conflict of interest statement
Dat Tran, Dan Palfrey, and Robert Welsh have no conflicts of interest to disclose.
Figures
Similar articles
-
Outcome and Cost of Optimal Control of Dyslipidemia in Adults With High Risk for Cardiovascular Disease.Can J Cardiol. 2021 Jan;37(1):66-76. doi: 10.1016/j.cjca.2020.03.022. Epub 2020 Mar 23. Can J Cardiol. 2021. PMID: 32738207
-
Resource Use and Burden of Hospitalization, Outpatient, Physician, and Drug Costs in Short- and Long-term Care After Acute Myocardial Infarction.Can J Cardiol. 2018 Oct;34(10):1298-1306. doi: 10.1016/j.cjca.2018.05.022. Epub 2018 Jun 5. Can J Cardiol. 2018. PMID: 30170782
-
The Healthcare Cost Burden of Acute Myocardial Infarction in Alberta, Canada.Pharmacoecon Open. 2018 Dec;2(4):433-442. doi: 10.1007/s41669-017-0061-0. Pharmacoecon Open. 2018. PMID: 29623635 Free PMC article.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
-
[Direct and indirect diabetes costs in the world].Medicina (Kaunas). 2004;40(1):16-26. Medicina (Kaunas). 2004. PMID: 14764977 Review. Lithuanian.
Cited by
-
The Potential Therapeutic Application of Simvastatin for Brain Complications and Mechanisms of Action.Pharmaceuticals (Basel). 2023 Jun 22;16(7):914. doi: 10.3390/ph16070914. Pharmaceuticals (Basel). 2023. PMID: 37513826 Free PMC article. Review.
-
Blood-Brain Barrier Permeability Is Associated With Cognitive Functioning in Normal Aging and Neurodegenerative Diseases.J Am Heart Assoc. 2024 Jul 16;13(14):e034225. doi: 10.1161/JAHA.124.034225. Epub 2024 Jul 9. J Am Heart Assoc. 2024. PMID: 38979810 Free PMC article.
-
Patients' health care resources utilization and costs estimation across cardiovascular risk categories: insights from the LATINO study.Health Econ Rev. 2024 Sep 12;14(1):73. doi: 10.1186/s13561-024-00550-2. Health Econ Rev. 2024. PMID: 39264520 Free PMC article.
-
Economic Evaluation of Population-Based BRCA1 and BRCA2 Testing in Canada.JAMA Netw Open. 2024 Sep 3;7(9):e2432725. doi: 10.1001/jamanetworkopen.2024.32725. JAMA Netw Open. 2024. PMID: 39264630 Free PMC article.
-
Advancing Cardiomyocyte Maturation: Current Strategies and Promising Conductive Polymer-Based Approaches.Adv Healthc Mater. 2024 May;13(13):e2303288. doi: 10.1002/adhm.202303288. Epub 2024 Feb 20. Adv Healthc Mater. 2024. PMID: 38349615 Free PMC article. Review.
References
-
- Public Health Agency of Canada. Tracking heart disease and stroke in Canada, 2009, viii. Ottawa: Public Health Agency of Canada; 2009.
-
- Grundy SM, et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;139(25):e1082–e1143. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
