

The Impact of Erythropoietin on Short- and Long-Term Kidney-Related Outcomes in Neonates of Extremely Low Gestational Age. Results of a Multicenter, Double-Blind, Placebo-Controlled Randomized Clinical Trial
- PMID: 33484699
- PMCID: PMC8093092
- DOI: 10.1016/j.jpeds.2021.01.031
The Impact of Erythropoietin on Short- and Long-Term Kidney-Related Outcomes in Neonates of Extremely Low Gestational Age. Results of a Multicenter, Double-Blind, Placebo-Controlled Randomized Clinical Trial
Abstract
Objective: To evaluate whether extremely low gestational age neonates (ELGANs) randomized to erythropoietin have better or worse kidney-related outcomes during hospitalization and at 22-26 months of corrected gestational age (cGA) compared with those randomized to placebo.
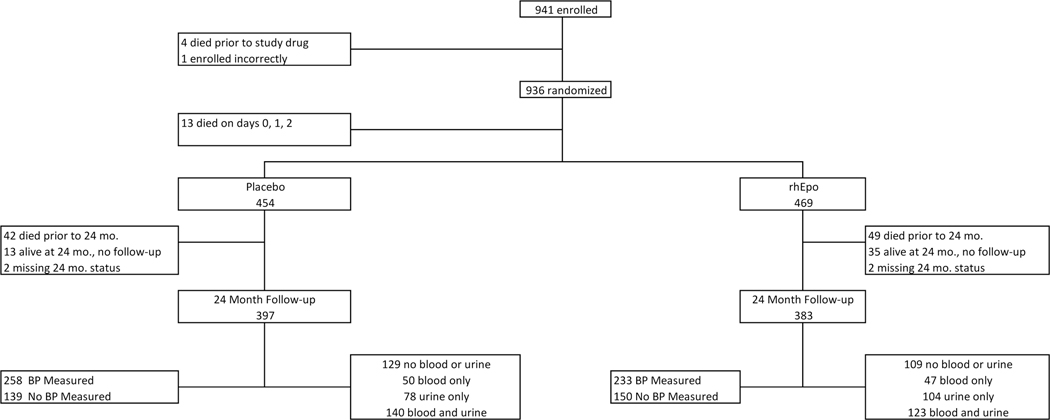
Study design: We performed an ancillary study to a multicenter double-blind, placebo-controlled randomized clinical trial of erythropoietin in ELGANs.
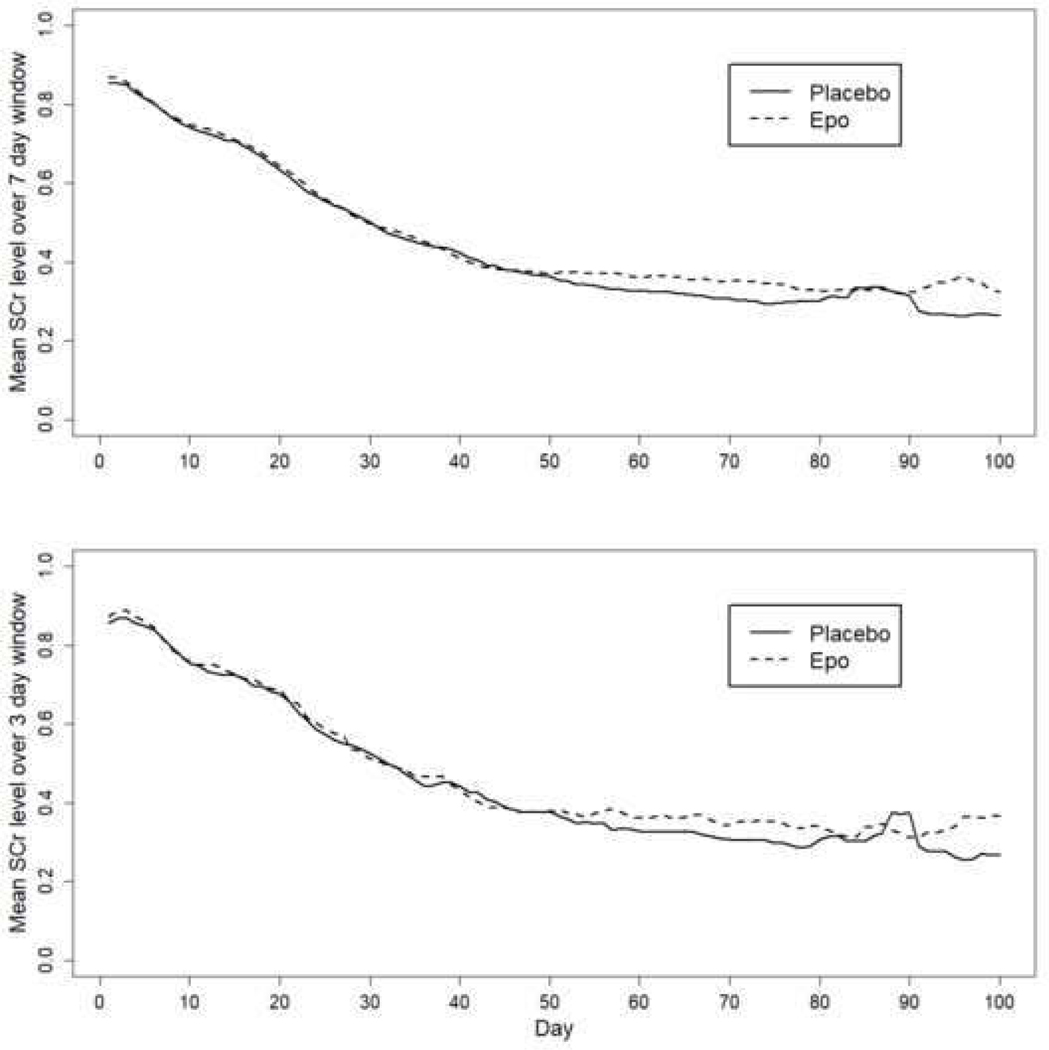
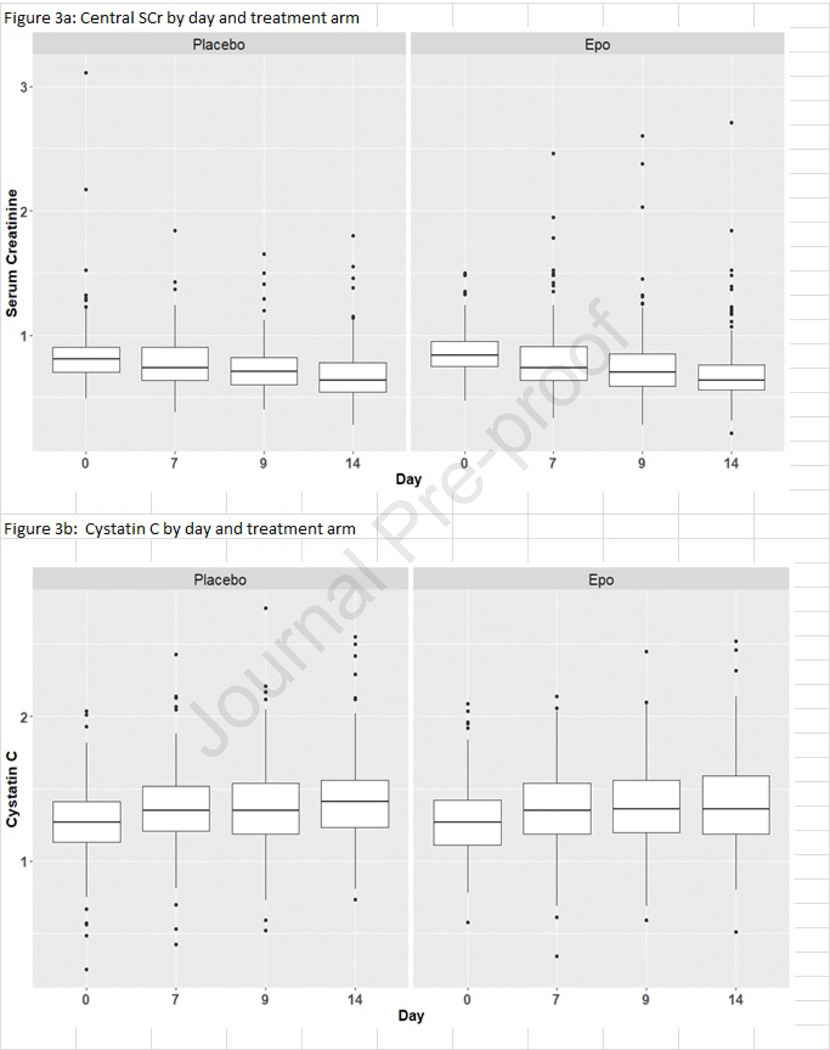
Results: The prevalence of severe (stage 2 or 3) acute kidney injury (AKI) was 18.2%. We did not find a statistically significant difference between those randomized to erythropoietin vs placebo for in-hospital primary (severe AKI) or secondary outcomes (any AKI and serum creatinine/cystatin C values at days 0, 7, 9, and 14). At 22-26 months of cGA, 16% of the cohort had an estimated glomerular filtration rate (eGFR) <90 mL/min/1.73 m2, 35.8% had urine albumin/creatinine ratio >30 mg/g, 23% had a systolic blood pressure (SBP) >95th percentile for age, and 40% had a diastolic blood pressure (DBP) >95th percentile for age. SBP >90th percentile occurred less often among recipients of erythropoietin (P < .04). This association remained even after controlling for gestational age, site, and sibship (aOR 0.6; 95% CI 0.39-0.92). We did not find statistically significant differences between treatment groups in eGFR, albumin/creatinine ratio, rates of SBP >95th percentile, or DBP >90th or >95th percentiles at the 2 year follow-up visit.
Conclusions: ELGANs have high rates of in-hospital AKI and kidney-related problems at 22-26 months of cGA. Recombinant erythropoietin may protect ELGANs against long-term elevated SBP but does not appear to protect from AKI, low eGFR, albuminuria, or elevated DBP at 22-26 months of cGA.
Keywords: acute kidney injury; acute renal failure; chronic kidney disease; hypertension; proteinuria.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
The other authors declare no conflicts of interest.
Figures
References
-
- Barker DJ, Martyn CN. The fetal origins of hypertension. Advances in nephrology from the Necker Hospital. 1997;26:65–72. - PubMed
-
- Xita N, Tsatsoulis A. Review: fetal programming of polycystic ovary syndrome by androgen excess: evidence from experimental, clinical, and genetic association studies. J Clin Endocrinol Metab. 2006;91:1660–6. - PubMed
-
- Fall CH, Barker DJ. The fetal origins of coronary heart disease and non-insulin dependent diabetes in India. Indian pediatrics. 1997;34:5–8. - PubMed
-
- Barker DJ. The fetal origins of coronary heart disease. Acta paediatrica. 1997;422:78–82. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
