

Radiological, epidemiological and clinical patterns of pulmonary viral infections
- PMID: 33485125
- PMCID: PMC7808729
- DOI: 10.1016/j.ejrad.2021.109548
Radiological, epidemiological and clinical patterns of pulmonary viral infections
Abstract
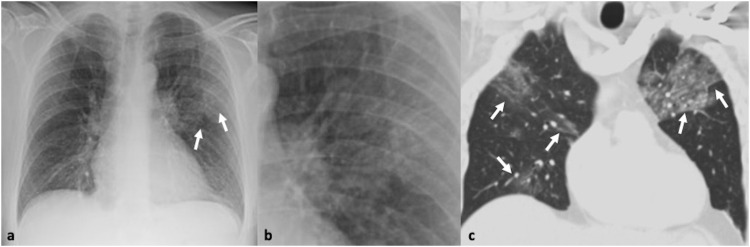
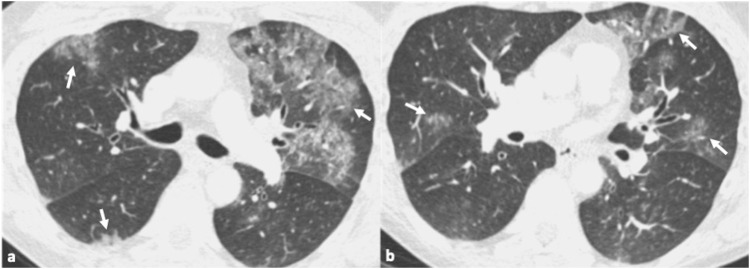
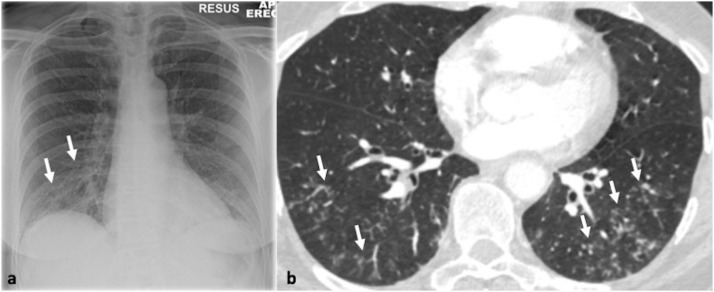
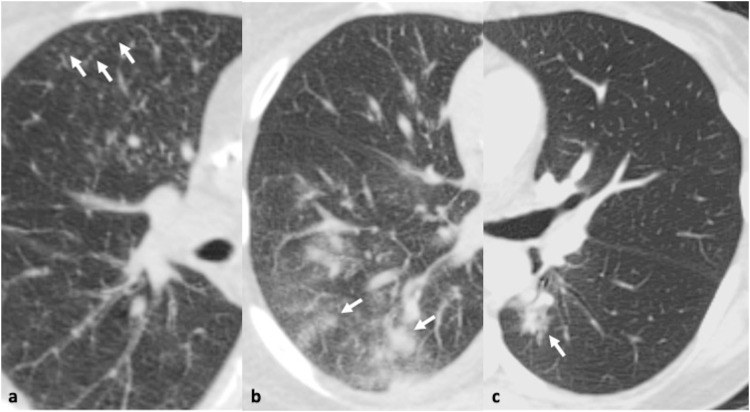
Respiratory viruses are the most common causes of acute respiratory infections. However, identification of the underlying viral pathogen may not always be easy. Clinical presentations of respiratory viral infections usually overlap and may mimic those of diseases caused by bacteria. However, certain imaging morphologic patterns may suggest a particular viral pathogen as the cause of the infection. Although definitive diagnosis cannot be made on the basis of clinical or imaging features alone, the use of a combination of clinical and radiographic findings can substantially improve the accuracy of diagnosis. The purpose of this review is to present the clinical, epidemiological and radiological patterns of lower respiratory tract viral pathogens providing a comprehensive approach for their diagnosis and identification in hospitals and community outbreaks.
Keywords: Chest x-ray; Clinical presentation; Computed Tomography; Diagnosis; Differential diagnosis; Epidemiology; Imaging; Respiratory viruses.
Copyright © 2021 Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors report no declarations of interest.
Figures

References
-
- Centers for Disease Control and Prevention, Past pandemics, Available at: https://www.cdc.gov/flu/pandemic-resources/basics/past-pandemics.html (Accessed 09 October 2020).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
