

Anemia as a risk factor for tuberculosis: a systematic review and meta-analysis
- PMID: 33485299
- PMCID: PMC7824931
- DOI: 10.1186/s12199-020-00931-z
Anemia as a risk factor for tuberculosis: a systematic review and meta-analysis
Abstract
Background: Tuberculosis is a major public health problem caused by Mycobacterium tuberculosis, occurring predominantly in population with low socioeconomic status. It is the second most common cause of death from infectious diseases. Tuberculosis becomes a double burden among anemic patients. Anemia increases an individual's susceptibility to infectious diseases including tuberculosis by reducing the immunity level. Therefore, the purpose of this study was to determine whether anemia is a risk factor for tuberculosis.
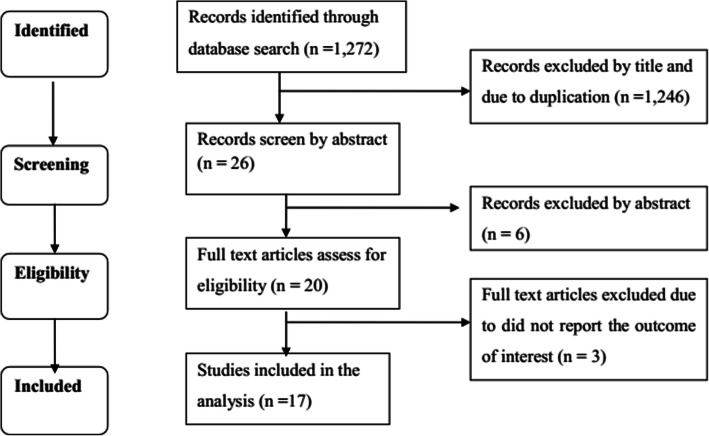
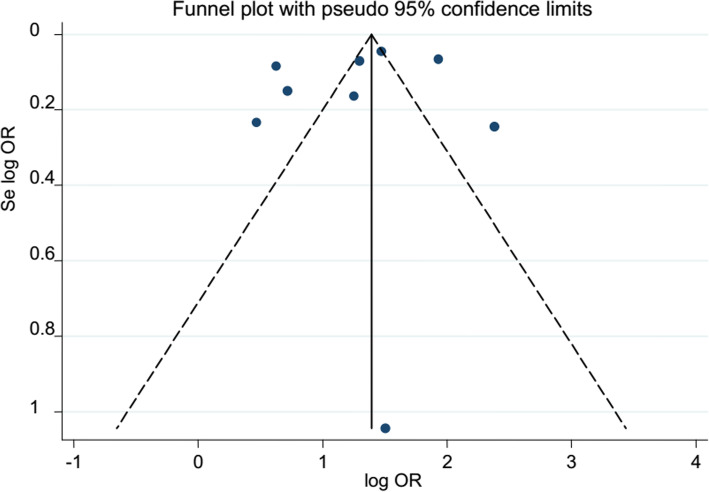
Method: Relevant published articles were searched in electronic databases like PubMed, Google Scholar, EMBASE, and Cochrane Library using the following MeSH terms: risk factor, predictors, tuberculosis, TB, Anaemia, Anemia, hemoglobin, Hgb, and Hb. Articles written in the English, observational studies conducted on the incidence/prevalence of tuberculosis among anemic patients, or papers examined anemia as risk factors for tuberculosis were included. From those studies meeting eligibility criteria, the first author's name, publication year, study area, sample size and age of participants, study design, and effect measure of anemia for tuberculosis were extracted. The data were entered using Microsoft Excel and exported to Stata version 11 for analysis. The random-effects model was applied to estimate the pooled OR and HR, and 95% CI. The sources of heterogeneity were tested by Cochrane I-squared statistics. The publication bias was assessed using Egger's test statistics.
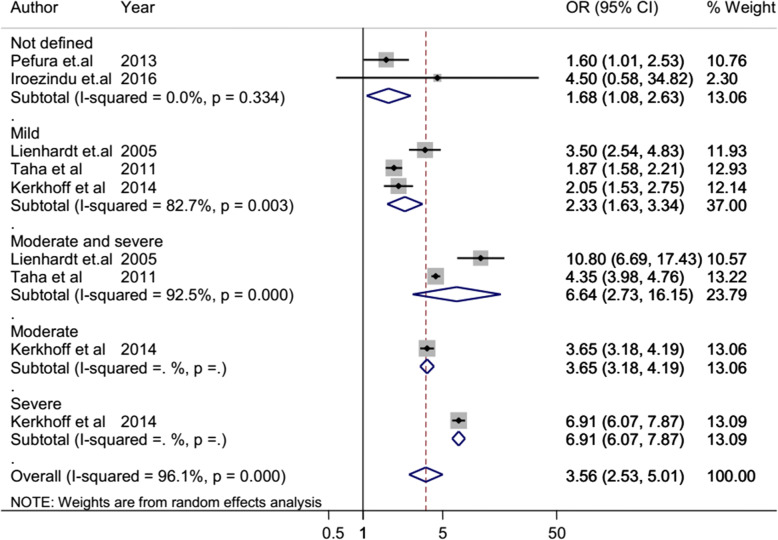
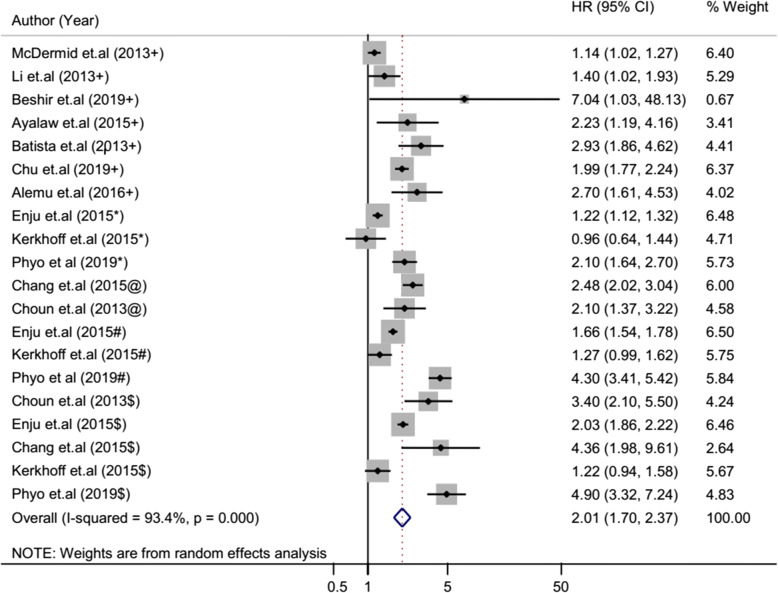
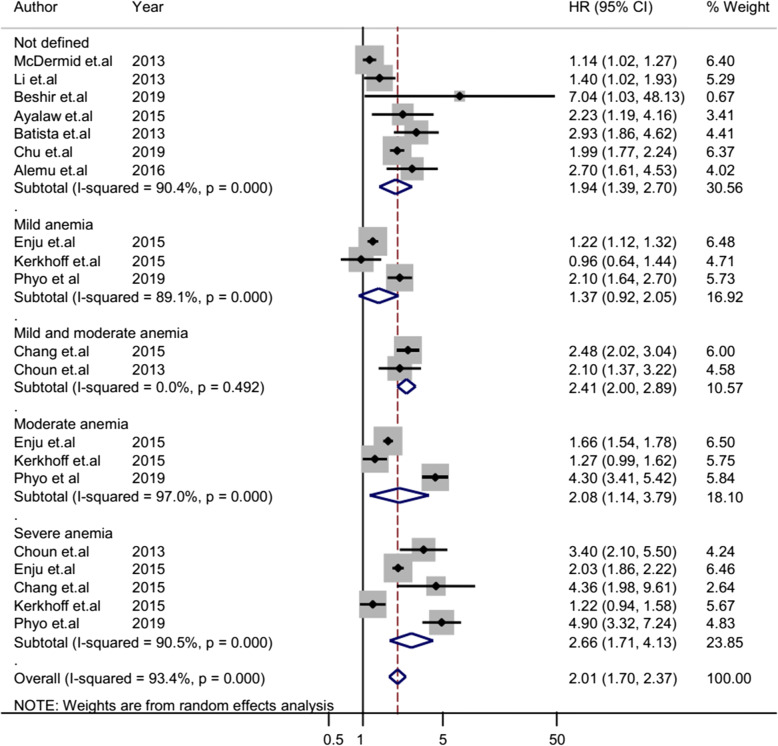
Results: A total of 17 articles with a 215,294 study participants were included in the analysis. The odd of tuberculosis among anemic patients was 3.56 (95% CI 2.53-5.01) times higher than non-anemic patients. The cohort studies showed that the HR of tuberculosis was 2.01 (95% CI 1.70-2.37) times higher among anemic patients than non-anemic patients. The hazard of tuberculosis also increased with anemia severity (HR 1.37 (95% CI 0.92-2.05), 2.08 (95% CI 1.14-3.79), and 2.66 (95% CI 1.71-4.13) for mild, moderate, and severe anemia, respectively).
Conclusion: According to the current systematic review and meta-analysis, we can conclude that anemia was a risk factor for tuberculosis. Therefore, anemia screening, early diagnose, and treatment should be provoked in the community to reduce the burden of tuberculosis.
Keywords: Anemia; Hazard ratio; Systematic review; Tuberculosis; and Meta-analysis.
Conflict of interest statement
The authors declare that they have competing interests.
Figures




References
-
- Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, et al. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. Lancet Glob Health. 2013;1(1):16–25. doi: 10.1016/S2214-109X(13)70001-9. - DOI - PMC - PubMed
-
- WHO, Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity; World Health Organization; Available from: https://www.who.int/vmnis/indicators/haemoglobin.pdf; Access date; October 20, 2020.
-
- De Benoist B, Cogswell M, Egli I, McLean E. Worldwide prevalence of anaemia 1993-2005. WHO Global Database of anaemia: World Health Organization; 2008. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical