

Global variation in postoperative mortality and complications after cancer surgery: a multicentre, prospective cohort study in 82 countries
- PMID: 33485461
- PMCID: PMC7846817
- DOI: 10.1016/S0140-6736(21)00001-5
Global variation in postoperative mortality and complications after cancer surgery: a multicentre, prospective cohort study in 82 countries
Erratum in
-
Department of Error.Lancet. 2021 Mar 6;397(10277):880. doi: 10.1016/S0140-6736(21)00456-6. Lancet. 2021. PMID: 33676626 Free PMC article. No abstract available.
Abstract
Background: 80% of individuals with cancer will require a surgical procedure, yet little comparative data exist on early outcomes in low-income and middle-income countries (LMICs). We compared postoperative outcomes in breast, colorectal, and gastric cancer surgery in hospitals worldwide, focusing on the effect of disease stage and complications on postoperative mortality.
Methods: This was a multicentre, international prospective cohort study of consecutive adult patients undergoing surgery for primary breast, colorectal, or gastric cancer requiring a skin incision done under general or neuraxial anaesthesia. The primary outcome was death or major complication within 30 days of surgery. Multilevel logistic regression determined relationships within three-level nested models of patients within hospitals and countries. Hospital-level infrastructure effects were explored with three-way mediation analyses. This study was registered with ClinicalTrials.gov, NCT03471494.
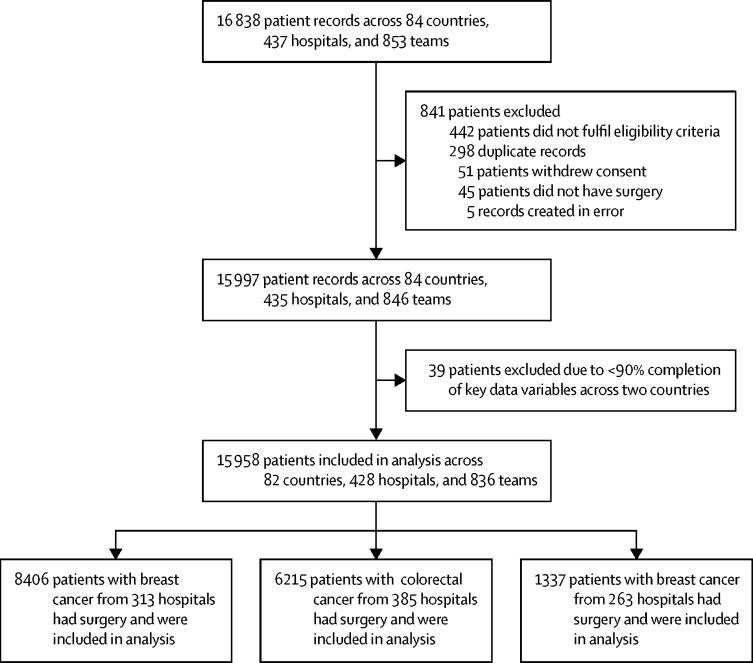
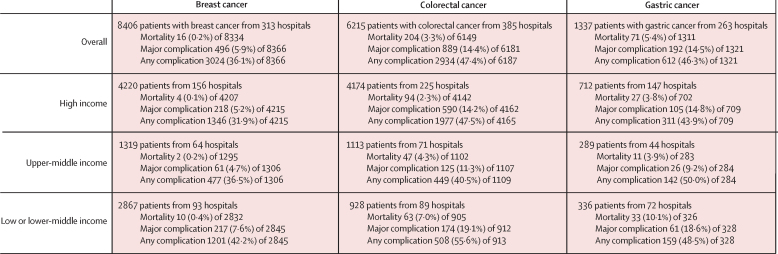
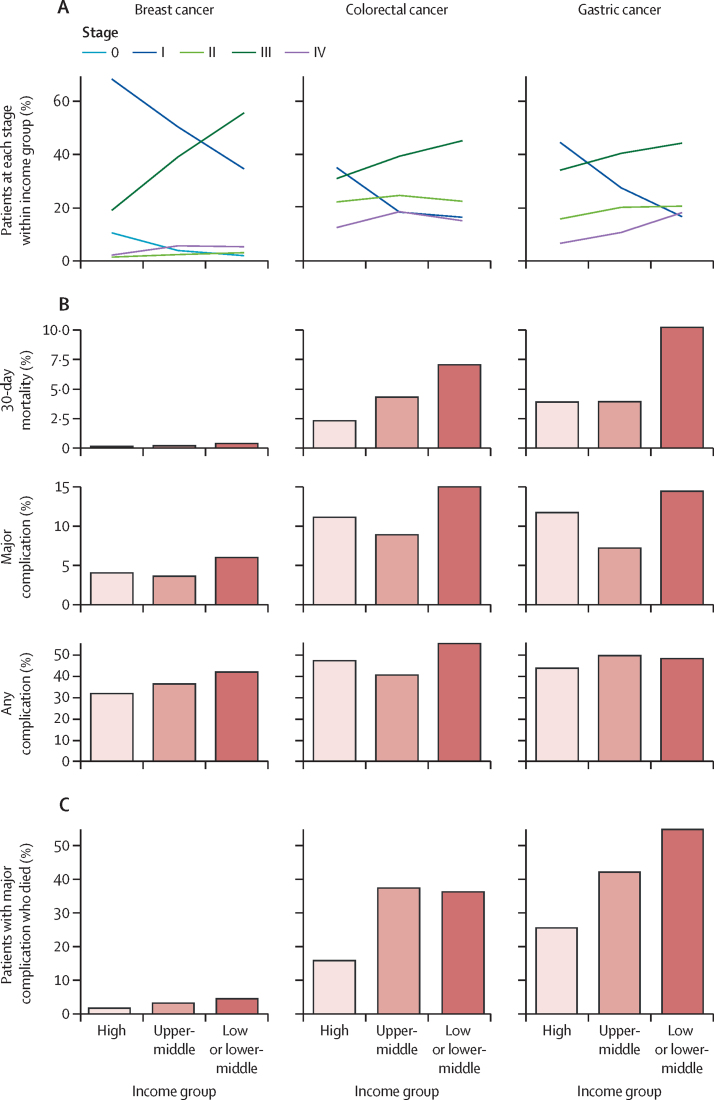
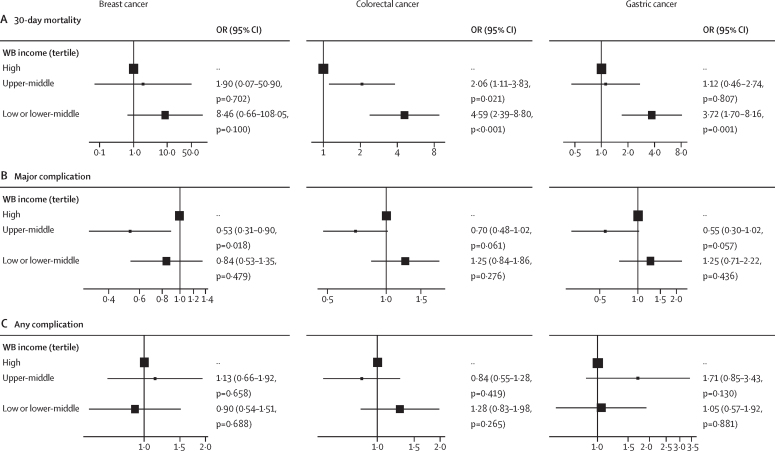
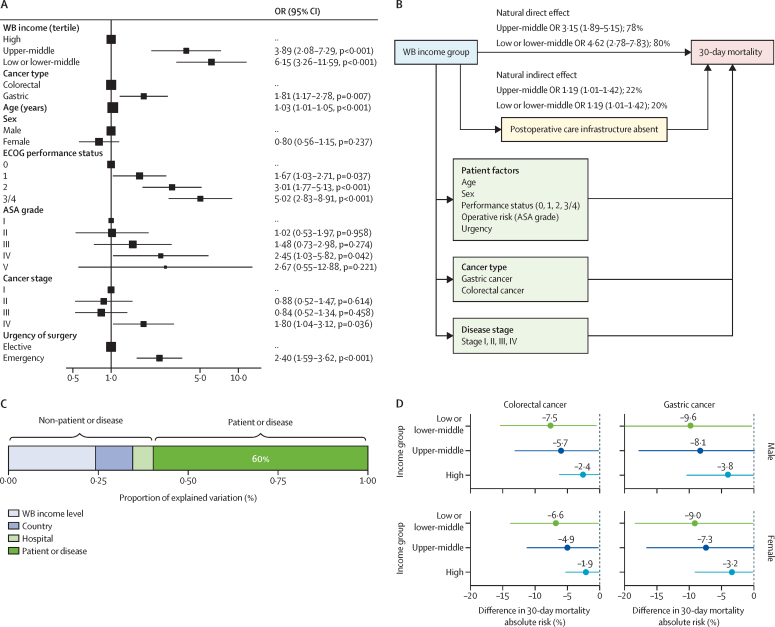
Findings: Between April 1, 2018, and Jan 31, 2019, we enrolled 15 958 patients from 428 hospitals in 82 countries (high income 9106 patients, 31 countries; upper-middle income 2721 patients, 23 countries; or lower-middle income 4131 patients, 28 countries). Patients in LMICs presented with more advanced disease compared with patients in high-income countries. 30-day mortality was higher for gastric cancer in low-income or lower-middle-income countries (adjusted odds ratio 3·72, 95% CI 1·70-8·16) and for colorectal cancer in low-income or lower-middle-income countries (4·59, 2·39-8·80) and upper-middle-income countries (2·06, 1·11-3·83). No difference in 30-day mortality was seen in breast cancer. The proportion of patients who died after a major complication was greatest in low-income or lower-middle-income countries (6·15, 3·26-11·59) and upper-middle-income countries (3·89, 2·08-7·29). Postoperative death after complications was partly explained by patient factors (60%) and partly by hospital or country (40%). The absence of consistently available postoperative care facilities was associated with seven to 10 more deaths per 100 major complications in LMICs. Cancer stage alone explained little of the early variation in mortality or postoperative complications.
Interpretation: Higher levels of mortality after cancer surgery in LMICs was not fully explained by later presentation of disease. The capacity to rescue patients from surgical complications is a tangible opportunity for meaningful intervention. Early death after cancer surgery might be reduced by policies focusing on strengthening perioperative care systems to detect and intervene in common complications.
Funding: National Institute for Health Research Global Health Research Unit.
Copyright © 2021 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
High burden of postoperative cancer mortality in LMICs.Lancet. 2021 Jan 30;397(10272):349-351. doi: 10.1016/S0140-6736(21)00187-2. Lancet. 2021. PMID: 33516321 No abstract available.
References
-
- Global Burden of Disease Cancer Collaboration. Fitzmaurice C, Allen C. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the Global Burden of Disease Study. JAMA Oncol. 2017;3:524. - PMC - PubMed
-
- Sullivan R, Alatise OI, Anderson BO. Global cancer surgery: delivering safe, affordable, and timely cancer surgery. Lancet Oncol. 2015;16:1193–1224. - PubMed
-
- Meara JG, Leather AJM, Hagander L. Global surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015;386:569–624. - PubMed
-
- Nepogodiev D, Moore R, Biccard B. Prioritizing research for patients requiring surgery in low- and middle-income countries. Br J Surg. 2019;106:e113–e120. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
