

Multi-Modal Analgesic Strategy for Trauma: A Pragmatic Randomized Clinical Trial
- PMID: 33486130
- PMCID: PMC7914202
- DOI: 10.1016/j.jamcollsurg.2020.12.014
Multi-Modal Analgesic Strategy for Trauma: A Pragmatic Randomized Clinical Trial
Abstract
Background: An effective strategy to manage acute pain and minimize opioid exposure is needed for injured patients. In this trial, we aimed to compare 2 multimodal pain regimens (MMPRs) for minimizing opioid exposure and relieving acute pain in a busy, urban trauma center.
Methods: This was an unblinded, pragmatic, randomized, comparative effectiveness trial of all adult trauma admissions except vulnerable patient populations and readmissions. The original MMPR (IV administration, followed by oral, acetaminophen, 48 hours of celecoxib and pregabalin, followed by naproxen and gabapentin, scheduled tramadol, and as-needed oxycodone) was compared with an MMPR of generic medications, termed the Multi-Modal Analgesic Strategies for Trauma (MAST) MMPR (ie oral acetaminophen, naproxen, gabapentin, lidocaine patches, and as-needed opioids). The primary endpoint was oral morphine milligram equivalents (MMEs) per day and secondary outcomes included total MMEs during hospitalization, opioid prescribing at discharge, and pain scores.
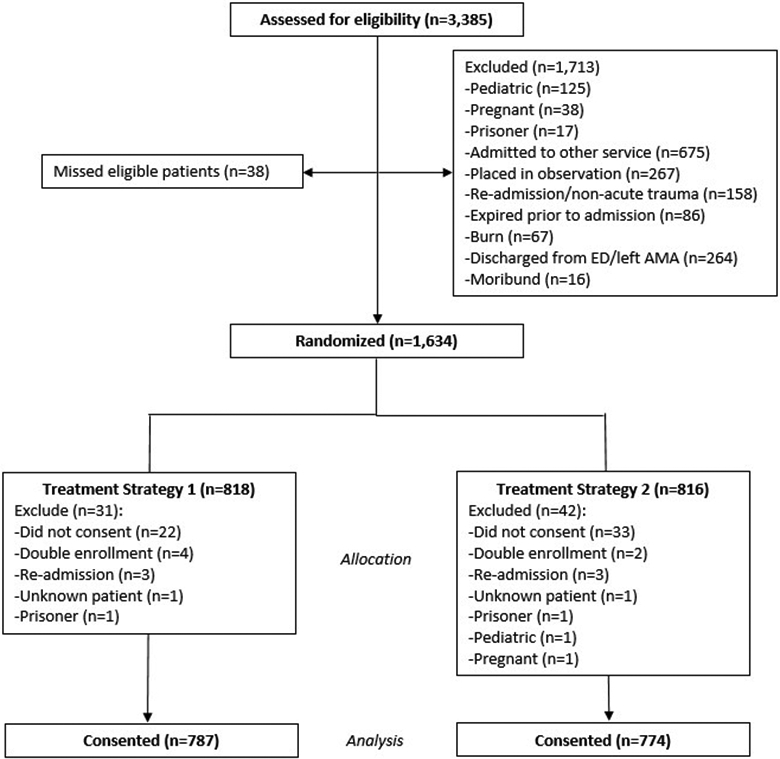
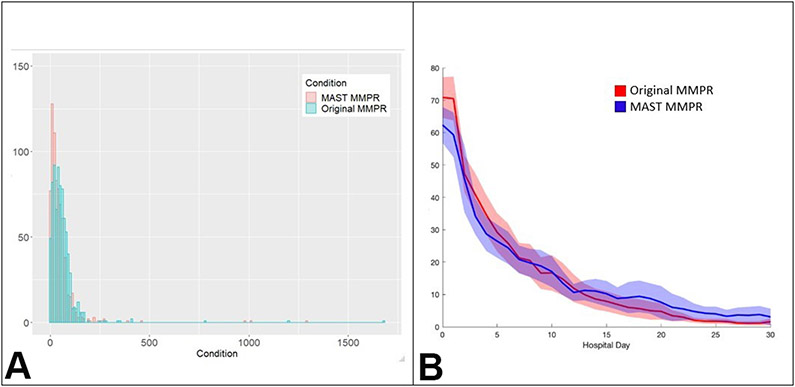
Results: During the trial, 1,561 patients were randomized, 787 to receive the original MMPR and 774 to receive the MAST MMPR. There were no differences in demographic characteristics, injury characteristics, or operations performed. Patients randomized to receive the MAST MMPR had lower MMEs per day (34 MMEs/d; interquartile range 15 to 61 MMEs/d vs 48 MMEs/d; interquartile range 22 to 74 MMEs/d; p < 0.001) and fewer were prescribed opioids at discharge (62% vs 67%; p = 0.029; relative risk 0.92; 95% credible interval, 0.86 to 0.99; posterior probability relative risk <1 = 0.99). No clinically significant difference in pain scores were seen.
Conclusions: The MAST MMPR was a generalizable and widely available approach that reduced opioid exposure after trauma and achieved adequate acute pain control.
Trial registration: ClinicalTrials.gov NCT03472469.
Copyright © 2020 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Pain Management in Trauma: Maximizing Multimodals to Minimize Opioids.J Am Coll Surg. 2021 Mar;232(3):251-252. doi: 10.1016/j.jamcollsurg.2020.12.020. J Am Coll Surg. 2021. PMID: 33637175 No abstract available.
References
-
- von Oelreich E, Eriksson M, Brattstrom O, et al. Risk factors and outcomes of chronic opioid use following trauma. Br J Surg. March 2020;107(4):413–21. - PubMed
-
- Wick EC, Grant MC, Wu CL. Postoperative Multimodal Analgesia Pain Management With Nonopioid Analgesics and Techniques: A Review. JAMA Surg. July 2017;152(7):691–7. - PubMed
-
- Pitchon DN, Dayan AC, Schwenk ES, et al. Updates on Multimodal Analgesia for Orthopedic Surgery. Anesthesiol Clin. September 2018;36(3):361–73. - PubMed
-
- Sim V, Hawkins S, Gave AA, et al. How low can you go: Achieving postoperative outpatient pain control without opioids. J Trauma Acute Care Surg. July 2019;87(1):100–3. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
