

The safety of outpatient total shoulder arthroplasty: a systematic review and meta-analysis
- PMID: 33486581
- PMCID: PMC7892728
- DOI: 10.1007/s00264-021-04940-7
The safety of outpatient total shoulder arthroplasty: a systematic review and meta-analysis
Abstract
Purpose: To meet the increasing demands of total shoulder arthroplasty (TSA) while reducing its financial burden, there has been a shift toward outpatient surgery. This systematic review and meta-analysis aimed to evaluate the safety of outpatient TSA.
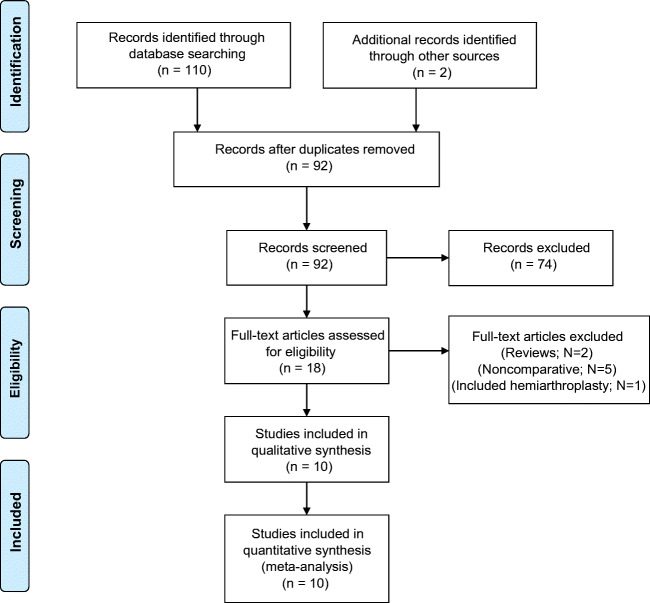
Methods: The primary objective was to compare re-admission rates and postoperative complications in outpatient versus inpatient TSA. The secondary objectives were functional outcomes and costs. PubMed, Google Scholar, and Web of Science were searched until March 28, 2020. The inclusion criteria were studies reporting at least complications or readmission rates within a period of 30 days or more.
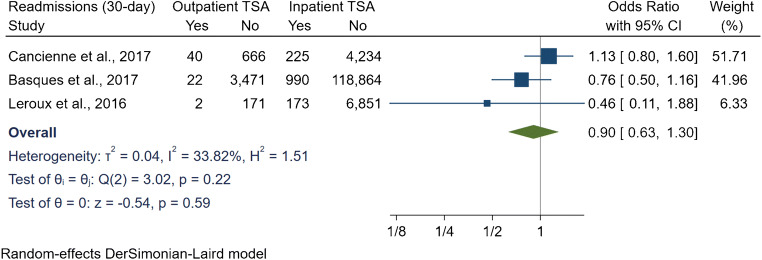
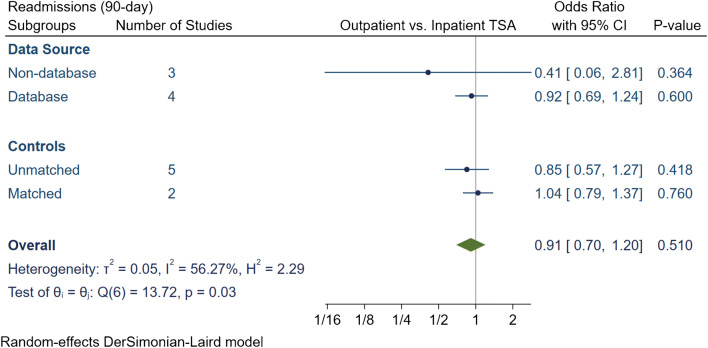
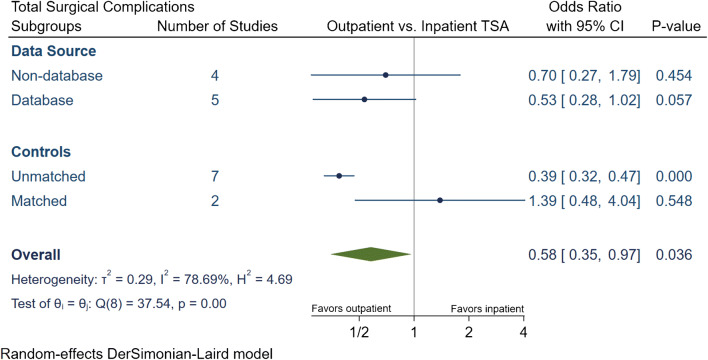
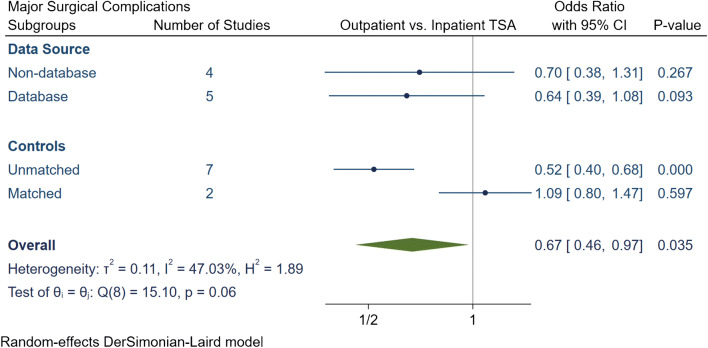
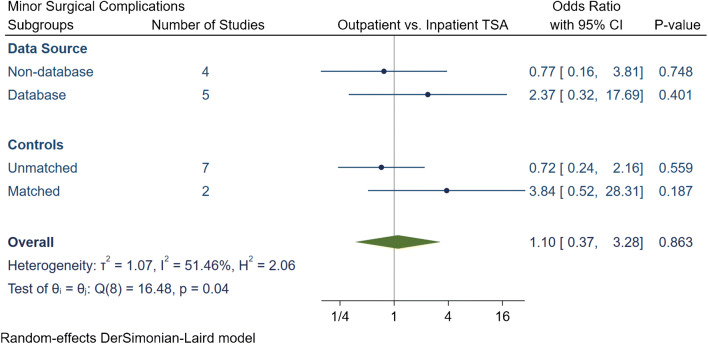
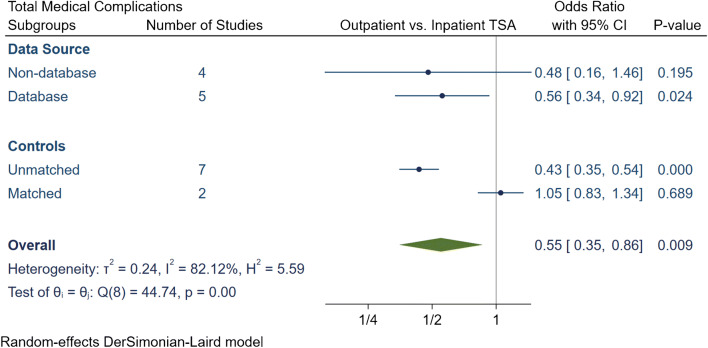
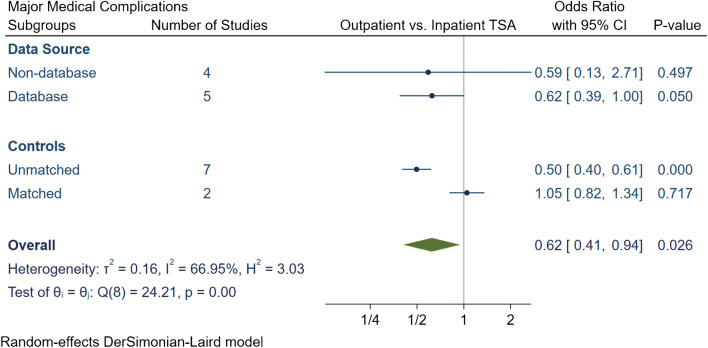
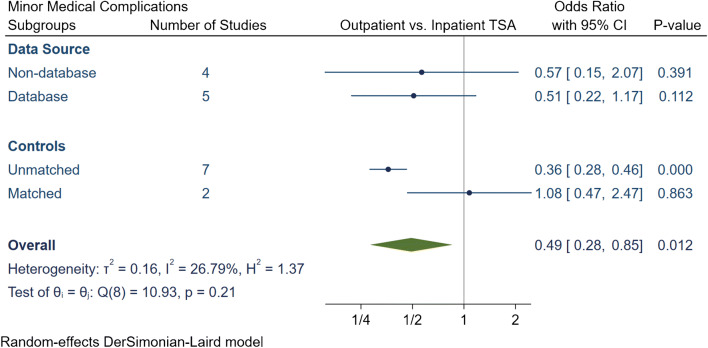
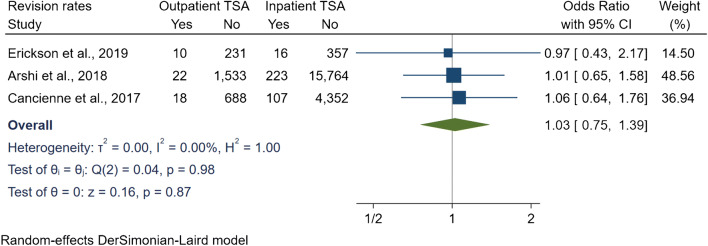
Results: Ten level III retrospective studies were included with 7637 (3.8%) and 192,025 (96.2%) patients underwent outpatient and inpatient TSA, respectively. Outpatient TSA had relatively younger and healthier patients. There were no differences between outpatient and inpatient arthroplasty for 30- and 90-day readmissions. Furthermore, unadjusted comparisons demonstrated significantly less total and major surgical complications, less total, major, and minor medical complications in favour of outpatient TSA. However, subgroup analyses demonstrated that there were no significant differences in all complication if the studies had matched controls and regardless of data source (database or nondatabase studies). The revision rates were similar between both groups at a 12-24 months follow-up. Two studies reported a significant reduction in costs in favour of outpatient TSA.
Conclusion: This study highlights that outpatient TSA could be a safe and effective alternative to inpatient TSA in appropriately selected patients. It was evident that outpatient TSA does not lead to increased readmissions, complications, or revision rates. A potential additional benefit of outpatient TSA was cost reduction.
Keywords: Ambulatory; Arthroplasty; Meta-analysis; Outpatient; Systematic review; Total shoulder.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Is outpatient shoulder arthroplasty safe? A systematic review and meta-analysis.J Shoulder Elbow Surg. 2021 Aug;30(8):1968-1976. doi: 10.1016/j.jse.2021.02.007. Epub 2021 Mar 4. J Shoulder Elbow Surg. 2021. PMID: 33675972
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
What is the optimal management of a loose glenoid component after anatomic total shoulder arthroplasty: a systematic review.J Shoulder Elbow Surg. 2023 Mar;32(3):653-661. doi: 10.1016/j.jse.2022.10.006. Epub 2022 Nov 4. J Shoulder Elbow Surg. 2023. PMID: 36343791
-
Safety and efficacy of outpatient hip and knee arthroplasty: a systematic review with meta-analysis.Arch Orthop Trauma Surg. 2022 Aug;142(8):1775-1791. doi: 10.1007/s00402-021-03811-5. Epub 2021 Feb 15. Arch Orthop Trauma Surg. 2022. PMID: 33587170
-
The transition to outpatient shoulder arthroplasty: a systematic review.J Shoulder Elbow Surg. 2022 Jul;31(7):e315-e331. doi: 10.1016/j.jse.2022.01.154. Epub 2022 Mar 9. J Shoulder Elbow Surg. 2022. PMID: 35278682
Cited by
-
Outpatient vs. inpatient total shoulder arthroplasty: complication rates, clinical outcomes, and eligibility parameters.JSES Int. 2023 Aug 22;8(3):483-490. doi: 10.1016/j.jseint.2023.06.029. eCollection 2024 May. JSES Int. 2023. PMID: 38707575 Free PMC article.
-
Trends in outpatient versus inpatient total shoulder arthroplasty over time.JSES Int. 2021 Nov 14;6(1):7-14. doi: 10.1016/j.jseint.2021.09.016. eCollection 2022 Jan. JSES Int. 2021. PMID: 35141669 Free PMC article.
-
Outpatient shoulder arthroplasty: An updated systematic review, meta-analysis, and trial sequential analysis on clinical outcomes and cost-effectiveness.Shoulder Elbow. 2025 Jun 25:17585732251349754. doi: 10.1177/17585732251349754. Online ahead of print. Shoulder Elbow. 2025. PMID: 40584214 Free PMC article. Review.
-
Comparison of Outcomes After Reverse Total Shoulder Arthroplasty in Patients With Proximal Humerus Fractures Versus Rotator Cuff Arthropathy.J Am Acad Orthop Surg Glob Res Rev. 2023 Oct 12;7(10):e23.00160. doi: 10.5435/JAAOSGlobal-D-23-00160. eCollection 2023 Oct 1. J Am Acad Orthop Surg Glob Res Rev. 2023. PMID: 37856701 Free PMC article.
-
Validated Wearable Device Shows Acute Postoperative Changes in Sleep Patterns Consistent With Patient-Reported Outcomes and Progressive Decreases in Device Compliance After Shoulder Surgery.Arthrosc Sports Med Rehabil. 2023 Aug 14;5(5):100783. doi: 10.1016/j.asmr.2023.100783. eCollection 2023 Oct. Arthrosc Sports Med Rehabil. 2023. PMID: 37636255 Free PMC article.
References
-
- Trofa D, Rajaee SS, Smith EL. Nationwide trends in total shoulder arthroplasty and hemiarthroplasty for osteoarthritis. Am J Orthop (Belle Mead NJ) 2014;43:166–172. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
