

One Giant Step for Giant Cell Arteritis: Updates in Diagnosis and Treatment
- PMID: 33488050
- PMCID: PMC7811148
- DOI: 10.1007/s11940-020-00660-2
One Giant Step for Giant Cell Arteritis: Updates in Diagnosis and Treatment
Abstract
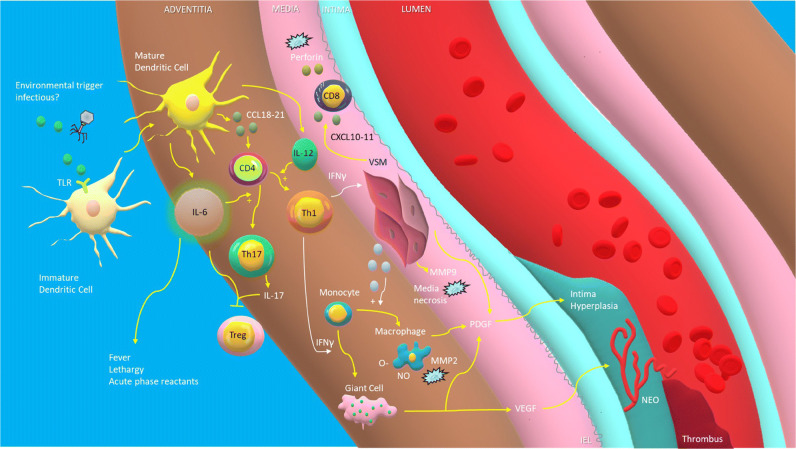
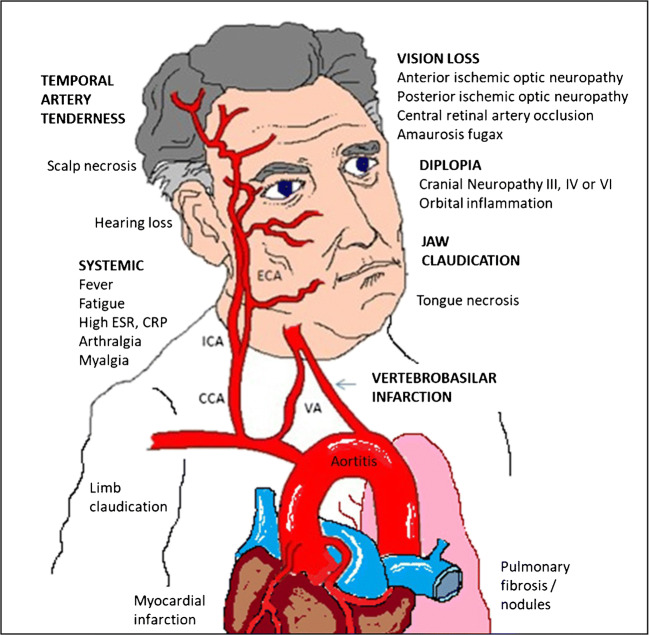
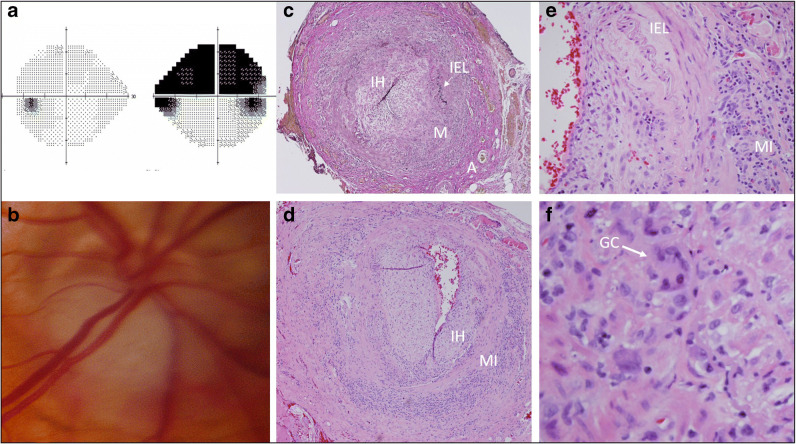
Purpose of review: Giant cell arteritis (GCA), a medium and large vessel vasculitis occurring in the aged, remains a formidable disease, capable of taking both vision and life, through a multitude of vascular complications. Our understanding of the spectrum of its manifestations has grown over the years, to include limb claudication, aortitis, and cardiac disease, in addition to the more classic visual complications resulting from of ischemia to branches of the external and internal carotid arteries. While a clinical presentation of headache, jaw claudication, scalp tenderness, fever and other systemic symptoms and serum markers are together highly suggestive of the disease, diagnosis can be challenging in those cases in which classic symptoms are lacking. The purpose of this review is to update the reader on advances in the diagnosis and treatment of giant cell arteritis and to review our evolving understanding of the immunological mechanism underlying the disease, which have helped guide our search for novel therapies.
Recent findings: There is increasing evidence supporting the use of Doppler ultrasound, dedicated post-contrast T1-weighted spin echo MRI of the scalp arteries and PET scan, which can together improve our diagnostic accuracy in cases in which temporal artery biopsy is either inconclusive or not feasible. Advances in our understanding of the immunological cascades underlying the disease have helped guide our search for steroid-sparing treatments for the GCA, the most important of which has been the IL-6 receptor antibody inhibitor tocilizumab, which has been shown to reduce cumulative steroid dose in a large multicenter, placebo-controlled prospective study. Other biologic agents, such as abatacept and ustekinumab have shown promise in smaller studies.
Summary: GCA is no longer a disease whose diagnosis is based exclusively on temporal artery biopsy and whose complications are prevented solely with the use of corticosteroids. Modern vascular imaging techniques and targeted immunologic therapies are heralding a new era for the disease, in which practitioners will hopefully be able to diagnosis it with greater accuracy and treat it with less ischemic complications and iatrogenic side effects.
Keywords: Anterior ischemic optic neuropathy; Doppler ultrasound; Giant cell arteritis; Granulomas; IL-6; Posterior ischemic optic neuropathy; Temporal arteritis; Tocilizumab; Vasculitis.
© The Author(s), under exclusive licence to Springer Science+Business Media, LLC part of Springer Nature 2021.
Figures
References
-
- Dumont A, Lecannuet A, Boutemy J, Maigné G, Martin-Silva N, Deshayes S, Audemard-Verger A, Sultan A, Planchard G, Aouba A, de Boysson H. Characteristics and outcomes of patients with ophthalmologic involvement in giant-cell arteritis: a case-control study. Semin Arthritis Rheum. 2020;50(2):335–341. doi: 10.1016/j.semarthrit.2019.09.008. - DOI - PubMed
-
- Horton BT, Magath TB, Brown GE. An undescribed form of arteritis of the temporal vessels. Proc Staff Meet Mayo Clinic. 1932;7:700–701.
-
- Hutchinson J. Diseases of the arteries, I.–on a peculiar form of thrombotic arteritis of the aged which is sometimes productive of gangrene. Arch Surg (London) 1890;1:323–329.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
