

Burden of Male Hypogonadism and Major Comorbidities, and the Clinical, Economic, and Humanistic Benefits of Testosterone Therapy: A Narrative Review
- PMID: 33488103
- PMCID: PMC7814241
- DOI: 10.2147/CEOR.S285434
Burden of Male Hypogonadism and Major Comorbidities, and the Clinical, Economic, and Humanistic Benefits of Testosterone Therapy: A Narrative Review
Abstract
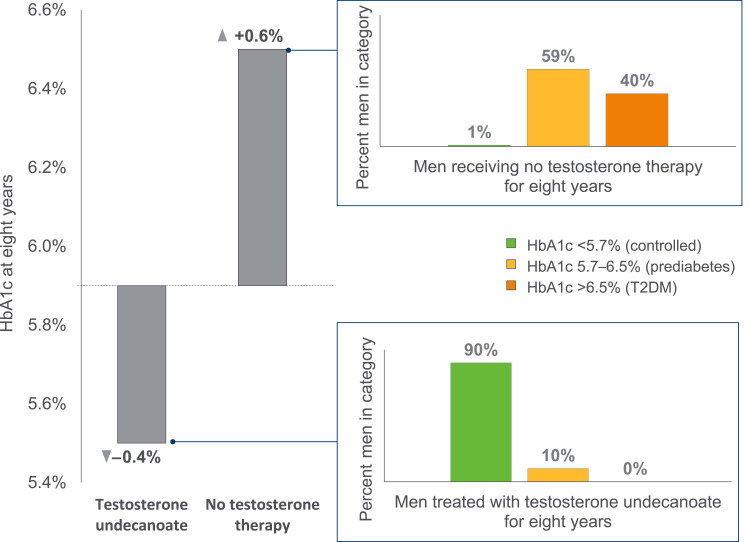
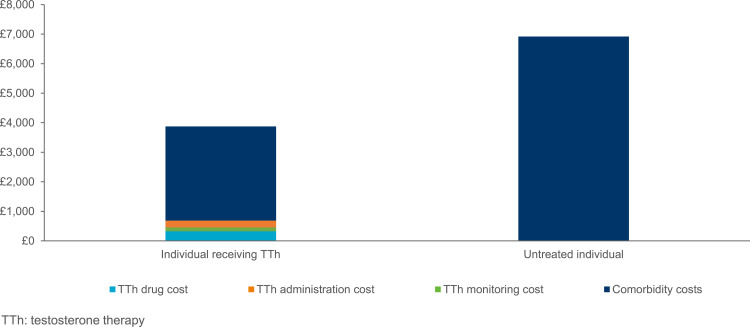
Male hypogonadism and major comorbidities such as type 2 diabetes mellitus, obesity, cardiovascular disease, and osteoporosis appear closely connected, forming a vicious cycle that leads to further hypogonadism. This narrative review provides a comprehensive overview of the current literature on the overall burden of male hypogonadism alongside related comorbidities, and how this may be alleviated through testosterone therapy. Observational and clinical data demonstrate that the interaction of male hypogonadism and its related comorbidities is associated with increased mortality, cardiovascular event risk and reduced quality of life. Evidence from epidemiological and registry-based studies shows that this clinical and humanistic burden translates to increased economic burden on health-care systems, through increased physician visits, medical claims, and drug costs. Male hypogonadism can be managed with testosterone therapy, which is intended to normalize testosterone concentrations and thereby reduce both hypogonadism symptoms and risk of comorbidities. Clinical and observational data suggest that in males with hypogonadism, testosterone therapy rapidly and sustainably improves glycemia, reduces risk of progression to diabetes, leads to significantly reduced waist circumference and fat mass, while providing significant positive effects on cardiovascular event risk and bone density. Significant and sustained improvement in patient-reported erectile function, urinary function, and aging male symptoms have also been shown. Economic evaluations have estimated that reduced comorbidity risk following testosterone therapy may lead to cost-savings, with one study estimating yearly inpatient savings of £3732 for treating comorbidities after intervention. A major unmet need exists in the area of male hypogonadism, particularly related to common comorbidities. Options for treatment include testosterone therapy, which has been shown to alleviate the clinical, economic, and humanistic burden associated with these conditions. As the prevalence of male hypogonadism is likely to increase globally, and this condition may be currently underdiagnosed, cost-saving testosterone therapies should be increasingly considered to manage hypogonadism.
Keywords: burden; cardiovascular disease; cost; hypogonadism; obesity; testosterone; type 2 diabetes.
© 2021 Yeo et al.
Conflict of interest statement
Sandy Yeo is an employee of Bayer, Singapore. Katsiaryna Holl, Nicolás Peñaherrera and Ulrike Wissinger are employees of Bayer, Germany. Kate Anstee and Robin Wyn are employees of Adelphi Values PROVE, who were commissioned by Bayer to conduct and report this research. The authors report no other conflicts of interest in this work.
Figures
Similar articles
-
Morbidity and mortality in men: Role of androgens.Best Pract Res Clin Endocrinol Metab. 2022 Jul;36(4):101662. doi: 10.1016/j.beem.2022.101662. Epub 2022 Apr 22. Best Pract Res Clin Endocrinol Metab. 2022. PMID: 35484028 Review.
-
Long-term testosterone treatment in elderly men with hypogonadism and erectile dysfunction reduces obesity parameters and improves metabolic syndrome and health-related quality of life.J Sex Med. 2014 Jun;11(6):1567-76. doi: 10.1111/jsm.12523. Epub 2014 Apr 8. J Sex Med. 2014. PMID: 24712761
-
Major cardiovascular disease risk in men with testosterone deficiency (hypogonadism): appraisal of short, medium and long-term testosterone therapy - a narrative review.Sex Med Rev. 2023 Sep 27;11(4):384-394. doi: 10.1093/sxmrev/qead031. Sex Med Rev. 2023. PMID: 37587664 Review.
-
A practical guide to male hypogonadism in the primary care setting.Int J Clin Pract. 2010 May;64(6):682-96. doi: 10.1111/j.1742-1241.2010.02355.x. Int J Clin Pract. 2010. PMID: 20518947 Free PMC article. Review.
-
Male-specific consequences of obesity - functional hypogonadism and fertility disorders.Endokrynol Pol. 2023;74(5):480-489. doi: 10.5603/ep.95626. Epub 2023 Oct 2. Endokrynol Pol. 2023. PMID: 37779374
Cited by
-
Testosterone and Covid-19: An update.Rev Med Virol. 2023 Jan;33(1):e2395. doi: 10.1002/rmv.2395. Epub 2022 Sep 3. Rev Med Virol. 2023. PMID: 36056748 Free PMC article. Review.
-
Reversible effect of castration induced hypogonadism on the morphology of the left coronary arteries in adult male rabbits.Anat Cell Biol. 2024 Mar 31;57(1):61-69. doi: 10.5115/acb.23.196. Epub 2023 Nov 30. Anat Cell Biol. 2024. PMID: 38030134 Free PMC article.
-
Testosterone replacement therapy in the era of telemedicine.Int J Impot Res. 2022 Nov;34(7):663-668. doi: 10.1038/s41443-021-00498-5. Epub 2021 Nov 19. Int J Impot Res. 2022. PMID: 34799712 Free PMC article. Review.
-
Effects on Bone and Muscle upon Treadmill Interval Training in Hypogonadal Male Rats.Biomedicines. 2023 May 5;11(5):1370. doi: 10.3390/biomedicines11051370. Biomedicines. 2023. PMID: 37239040 Free PMC article.
-
The Burden of Hormonal Disorders: A Worldwide Overview With a Particular Look in Italy.Front Endocrinol (Lausanne). 2021 Jun 16;12:694325. doi: 10.3389/fendo.2021.694325. eCollection 2021. Front Endocrinol (Lausanne). 2021. PMID: 34220719 Free PMC article. Review.
References
-
- Traish AM. Negative Impact of Testosterone Deficiency and 5alpha-Reductase Inhibitors Therapy on Metabolic and Sexual Function in Men. Adv Exp Med Biol. 2017;1043:473–526. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
