

Survey of Paediatric Oncologists and Pathologists regarding Their Views and Experiences with Variant Translocations in Ewing and Ewing-Like Sarcoma: A Report of the Children's Oncology Group
- PMID: 33488267
- PMCID: PMC7787769
- DOI: 10.1155/2020/3498549
Survey of Paediatric Oncologists and Pathologists regarding Their Views and Experiences with Variant Translocations in Ewing and Ewing-Like Sarcoma: A Report of the Children's Oncology Group
Abstract
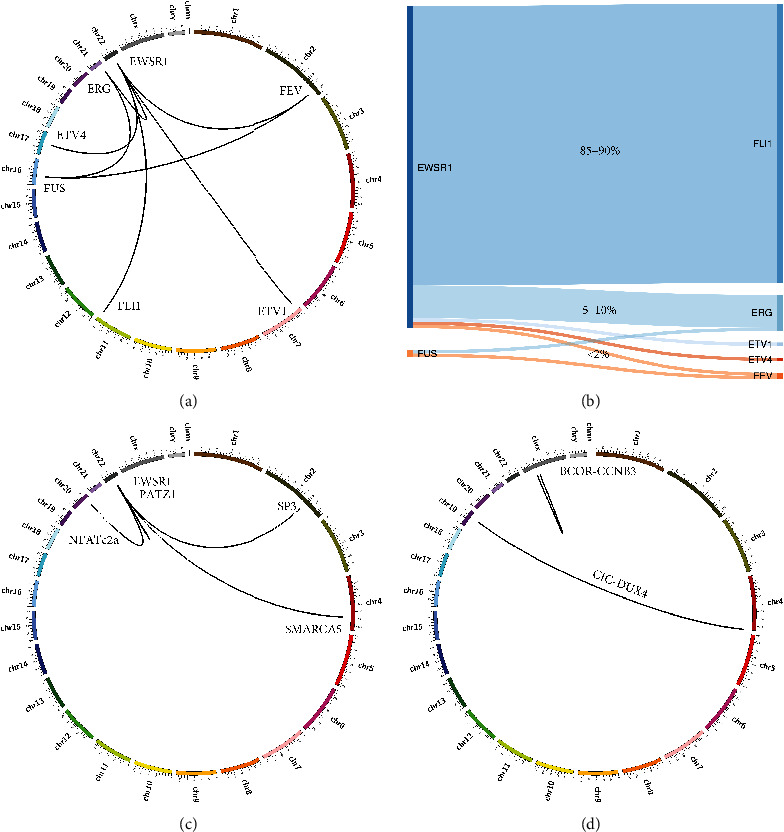
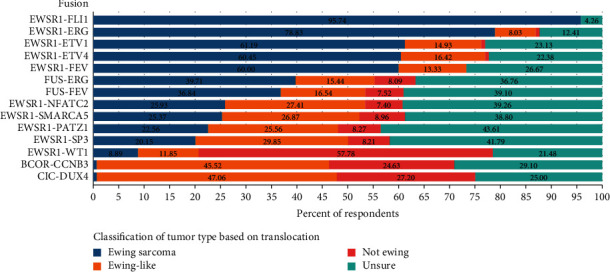
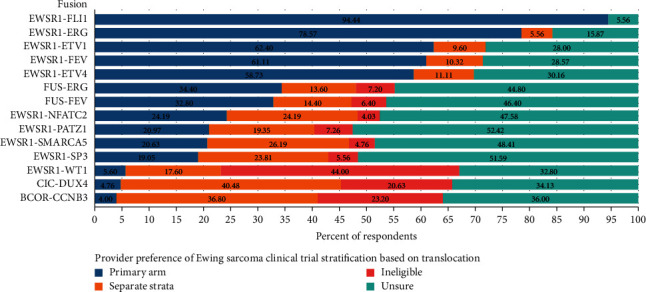
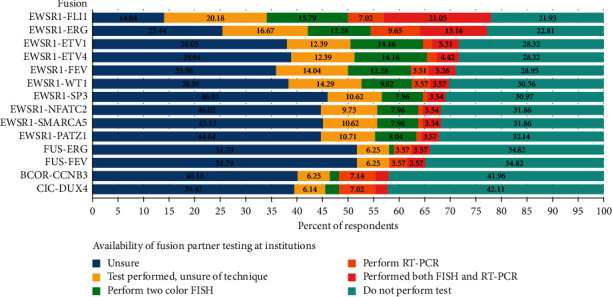
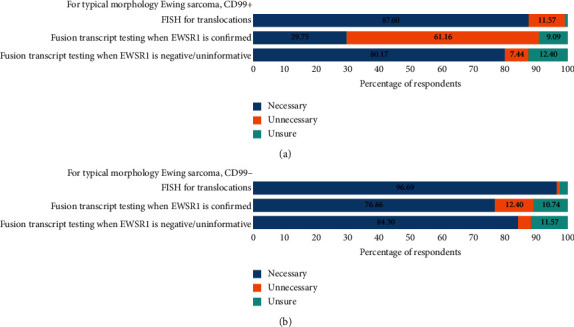
Advances in molecular diagnostics have identified subsets of Ewing and Ewing-like sarcomas driven by variant translocations with unique biology. It is likely that patients with these tumours will have different clinical features and therapeutic outcomes. Nevertheless, the management of these patients both locally and within cooperative group trials depends on the local pathological diagnosis. It is not known what molecular diagnostic approaches are employed by local pathologists or if the exact translocation is commonly determined. In addition, it is not known what therapeutic approaches are employed for these patients or what cooperative trials are deemed appropriate for these patients by expert consensus. To answer these questions, we performed an international survey of oncologists and pathologists to better understand the diagnostic approaches used to identify variant translocations and the influence the findings have on therapy and clinical trial eligibility. An online survey was distributed to oncologists and pathologists primarily in North America. A total of 141 surveys were completed, representing a 28% response rate. The majority of respondents considered EWSR1-ETS gene family translocations (range 61-96%) to be Ewing sarcoma and would include them on the primary arm of a Ewing sarcoma clinical trial. There was a lack of consensus on how to classify and stratify BCOR-CCNB3, CIC-DUX4, and EWSR1+ with non-ETS partner fusions. Most respondents were either unsure how their institution tested, or their institution did not perform the test. In cases with atypical Ewing morphology, most respondents favoured additional fusion transcript testing. There is a lack of consensus regarding the classification and stratification of rare molecular subtypes in Ewing sarcoma. It is not clear how these alternative translocations have impacted outcomes for past clinical studies. This suggests a need for molecular confirmation of diagnoses and centralized or minimum standardization of testing for future trial enrolment.
Copyright © 2020 Michael D. Kinnaman et al.
Conflict of interest statement
K.A. Janeway has received consulting fees from Bayer. S.L. Lessnick is a scientific advisor for Salarius Pharmaceuticals and has patents related to NKX2.2 and GSTM4 in Ewing sarcoma.
Figures
References
-
- Jeon I. S., Davis J. N., Braun B. S., et al. A variant Ewing’s sarcoma translocation (7;22) fuses the EWS gene to the ETS gene ETV1. Oncogene. 1995;10(6):1229–1234. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
