

Pluripotential Risk and Clinical Staging: Theoretical Considerations and Preliminary Data From a Transdiagnostic Risk Identification Approach
- PMID: 33488413
- PMCID: PMC7819892
- DOI: 10.3389/fpsyt.2020.553578
Pluripotential Risk and Clinical Staging: Theoretical Considerations and Preliminary Data From a Transdiagnostic Risk Identification Approach
Abstract
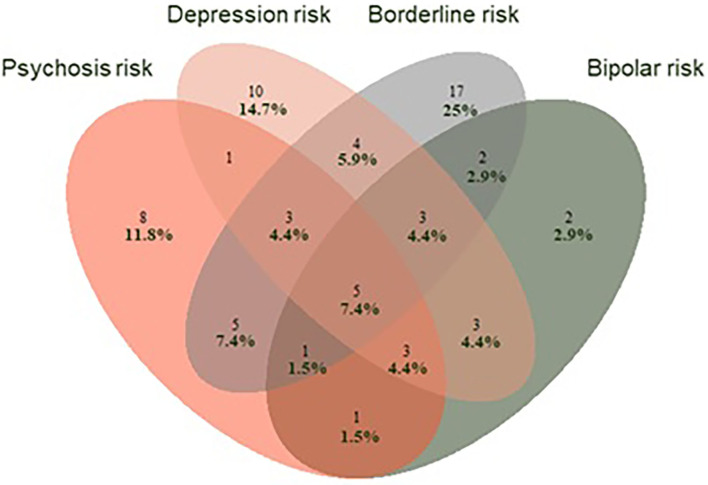
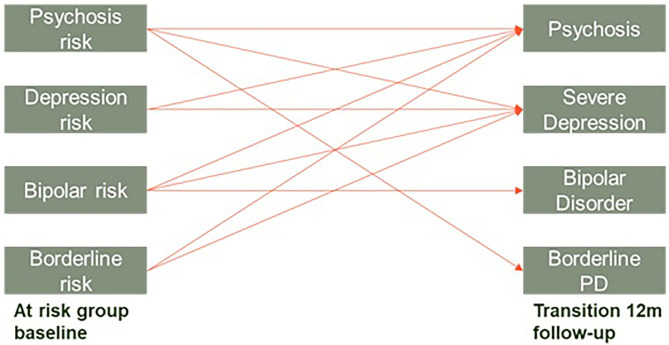
Most psychiatric disorders develop during adolescence and young adulthood and are preceded by a phase during which attenuated or episodic symptoms and functional decline are apparent. The introduction of the ultra-high risk (UHR) criteria two decades ago created a new framework for identification of risk and for pre-emptive psychiatry, focusing on first episode psychosis as an outcome. Research in this paradigm demonstrated the comorbid, diffuse nature of emerging psychopathology and a high degree of developmental heterotopy, suggesting the need to adopt a broader, more agnostic approach to risk identification. Guided by the principles of clinical staging, we introduce the concept of a pluripotent at-risk mental state. The clinical high at risk mental state (CHARMS) approach broadens identification of risk beyond psychosis, encompassing multiple exit syndromes such as mania, severe depression, and personality disorder. It does not diagnostically differentiate the early stages of psychopathology, but adopts a "pluripotent" approach, allowing for overlapping and heterotypic trajectories and enabling the identification of both transdiagnostic and specific risk factors. As CHARMS is developed within the framework of clinical staging, clinical utility is maximized by acknowledging the dimensional nature of clinical phenotypes, while retaining thresholds for introducing specific interventions. Preliminary data from our ongoing CHARMS cohort study (N = 114) show that 34% of young people who completed the 12-month follow-up assessment (N = 78) transitioned from Stage 1b (attenuated syndrome) to Stage 2 (full disorder). While not without limitations, this broader risk identification approach might ultimately allow reliable, transdiagnostic identification of young people in the early stages of severe mental illness, presenting further opportunities for targeted early intervention and prevention strategies.
Keywords: at risk mental state; at-risk (youth); clinical staging model; pluripotency; transdiagnostic.
Copyright © 2021 Hartmann, McGorry, Destree, Amminger, Chanen, Davey, Ghieh, Polari, Ratheesh, Yuen and Nelson.
Conflict of interest statement
PM reported receiving grant funding from National Alliance for Research on Schizophrenia and Depression and unrestricted research funding from AstraZeneca, Eli Lilly, Janssen-Cilag, Pfizer, and Novartis, as well as honoraria for educational activities with AstraZeneca, Eli Lilly, Janssen-Cilag, Pfizer, Bristol-Myers Squibb, Roche, and the Lundbeck Institute. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Mei C, Nelson B, Hartmann J, Spooner R, McGorry PD. Chapter 4 - Transdiagnostic early intervention, prevention, and prediction in psychiatry. In: Baune BT, editor. Personalized Psychiatry. San Diego: Academic Press, 27–37.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials