

Occupational hazard in an immunosuppressed patient
- PMID: 33489071
- PMCID: PMC7802483
- DOI: 10.1136/flgastro-2019-101221
Occupational hazard in an immunosuppressed patient
Abstract
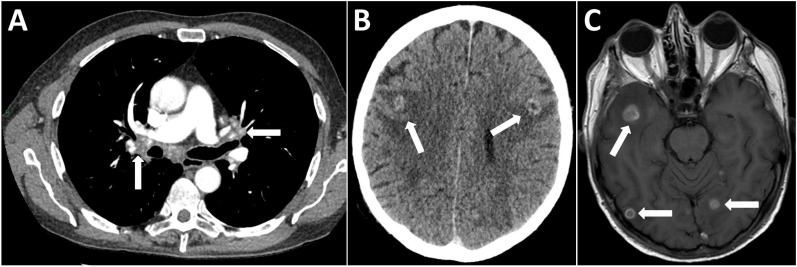
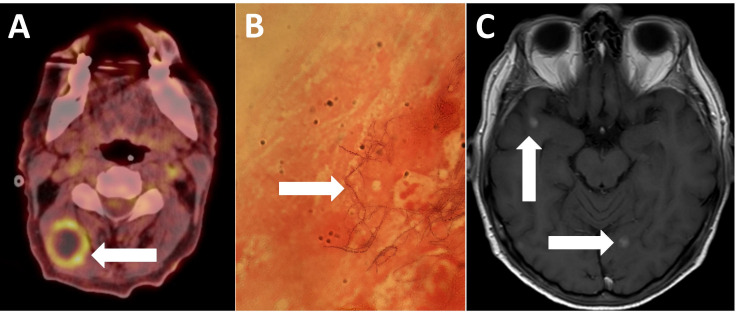
A 60-year-old male liver transplant recipient presented to his local hospital with left-sided partial seizures following a few days of generalised headache. He had undergone transplantation for primary sclerosing cholangitis 4 years earlier and maintained on tacrolimus monotherapy immunosuppression. He had no other comorbidities of note and worked as an arable farmer. At last follow-up, he had been well with preserved graft function and afternoon trough tacrolimus levels of 2-4 ng/mL. Over the preceding 4 weeks, he had been investigated locally for weight loss and a productive cough, where CT of the chest showed calcified mediastinal and hilar lymphadenopathy. Bronchoscopy samples were negative for acid-fast bacilli and he had been empirically treated for assumed community acquired pneumonia. Initial seizure management was with intravenous diazepam and phenytoin. On transfer to our centre, he was noted to be dysarthric with persisting 4/5 left upper limb weakness and nystagmus to all extremes of gaze. Blood tests were significant for mild anaemia (haemoglobin 90 g/L) and elevated C reactive protein (134 mg/L). The peripheral white cell count was 6.6×109/L. Biochemical liver graft function was normal and the 8am trough tacrolimus level was low at 2 ng/mL. CT head revealed bilateral ring enhancing cerebral lesions with surrounding vasogenic oedema but no mass effect. On MRI these exhibited restricted diffusion and marked perilesional oedema, suggestive of infection. Cerebrospinal fluid (CSF) analysis was as follows: white cell count <1/mm3, protein 0.57 g/L (normal range <45 g/L) and glucose 3 mmol/L (paired plasma glucose 4.8 mmol/L). Testing for virological causes via PCR, toxoplasma serology and blood and CSF cultures, including for tuberculosis, were all negative. Whole body positron emission tomography-CT demonstrated uptake in numerous peritoneal and intramuscular lesions as well as right-sided cervical lymphadenopathy, which was sampled with fine needle aspiration. Microscopy revealed a filamentous, beading and branching Gram-positive bacillus that was partially acid-fast, subsequently speciated as Nocardia farcinica.
Keywords: infectious disease; liver; orthotopic liver transplantation.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

References
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials