

Face coverings and respiratory tract droplet dispersion
- PMID: 33489292
- PMCID: PMC7813263
- DOI: 10.1098/rsos.201663
Face coverings and respiratory tract droplet dispersion
Abstract
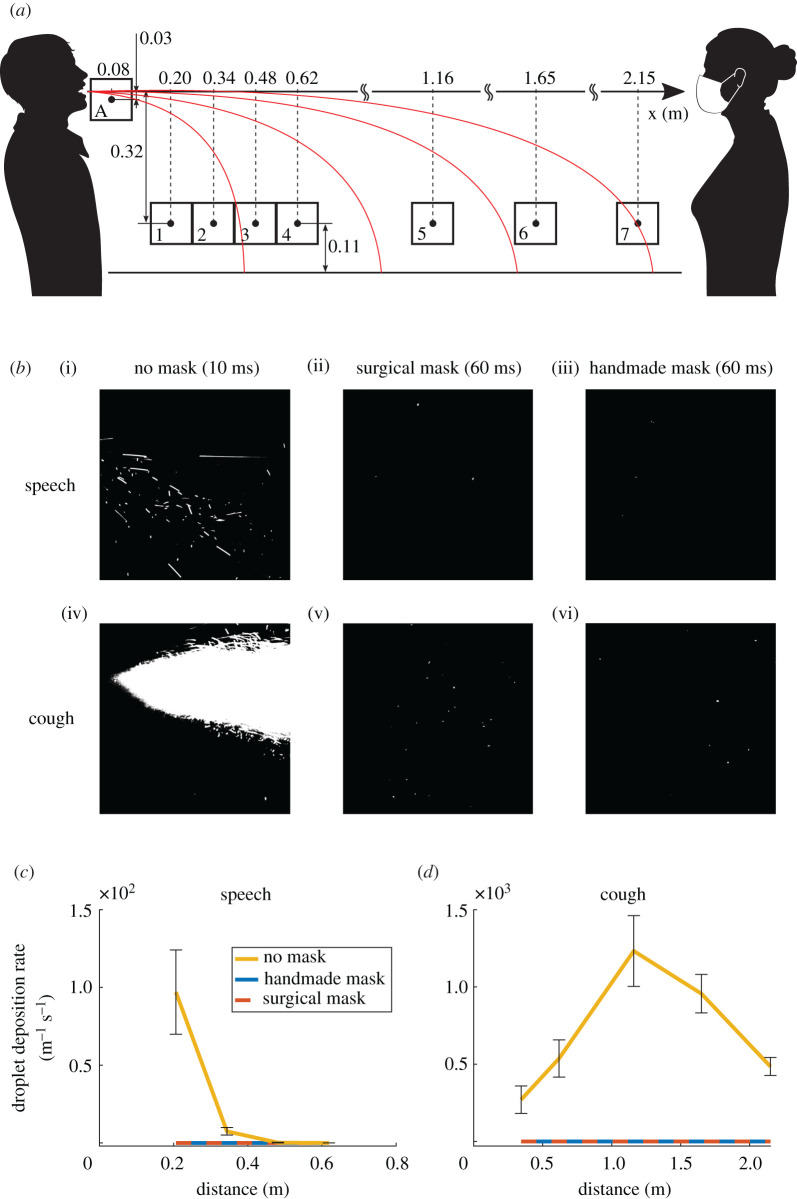
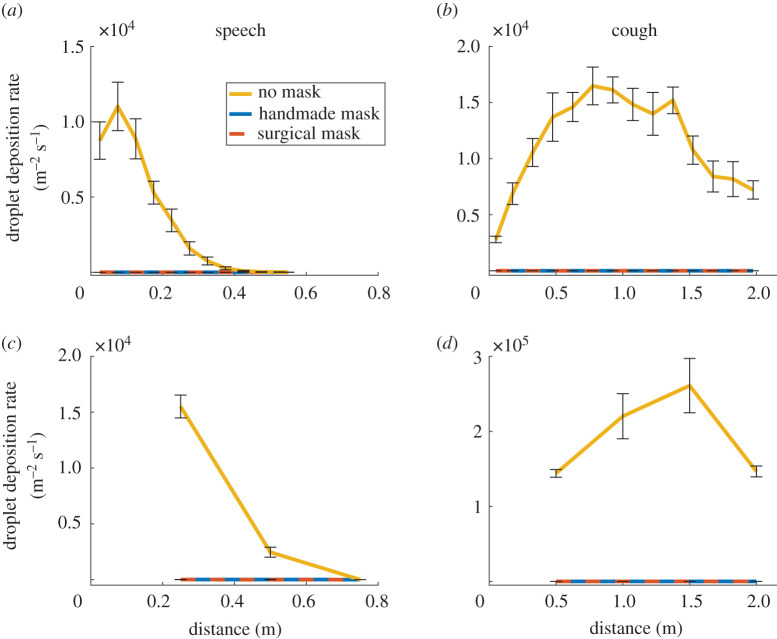
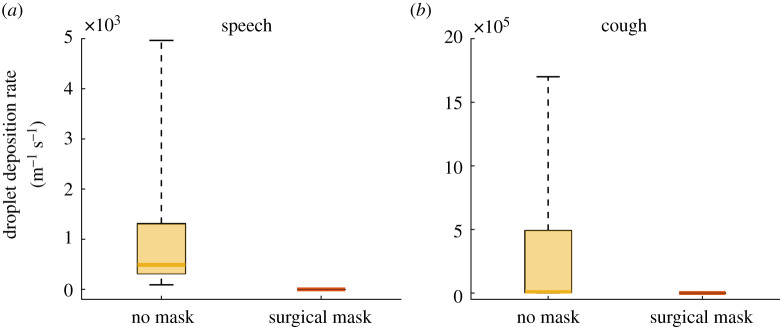
Respiratory droplets are the primary transmission route for SARS-CoV-2, a principle which drives social distancing guidelines. Evidence suggests that virus transmission can be reduced by face coverings, but robust evidence for how mask usage might affect safe distancing parameters is lacking. Accordingly, we set out to quantify the effects of face coverings on respiratory tract droplet deposition. We tested an anatomically realistic manikin head which ejected fluorescent droplets of water and human volunteers, in speaking and coughing conditions without a face covering, or with a surgical mask or a single-layer cotton face covering. We quantified the number of droplets in flight using laser sheet illumination and UV-light for those that had landed at table height at up to 2 m. For human volunteers, expiratory droplets were caught on a microscope slide 5 cm from the mouth. Whether manikin or human, wearing a face covering decreased the number of projected droplets by less than 1000-fold. We estimated that a person standing 2 m from someone coughing without a mask is exposed to over 10 000 times more respiratory droplets than from someone standing 0.5 m away wearing a basic single-layer mask. Our results indicate that face coverings show consistent efficacy at blocking respiratory droplets and thus provide an opportunity to moderate social distancing policies. However, the methodologies we employed mostly detect larger (non-aerosol) sized droplets. If the aerosol transmission is later determined to be a significant driver of infection, then our findings may overestimate the effectiveness of face coverings.
Keywords: COVID-19; face covering; handmade mask; respiratory droplets; social distancing; surgical mask.
© 2020 The Authors.
Conflict of interest statement
We declare we have no competing interests.
Figures
References
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous