

Vitamin D and COVID-19: evidence and recommendations for supplementation
- PMID: 33489300
- PMCID: PMC7813231
- DOI: 10.1098/rsos.201912
Vitamin D and COVID-19: evidence and recommendations for supplementation
Abstract
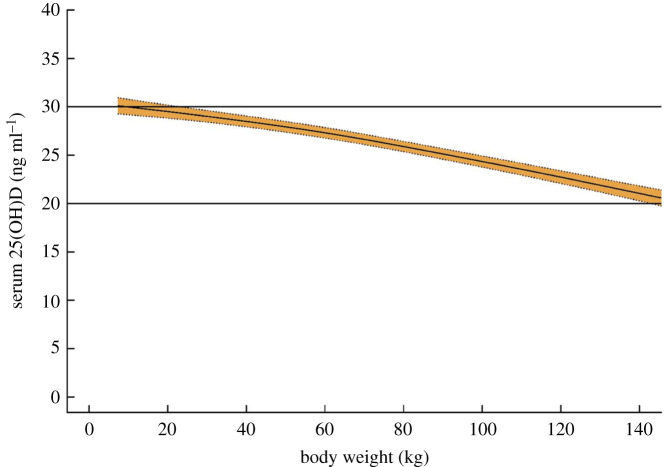
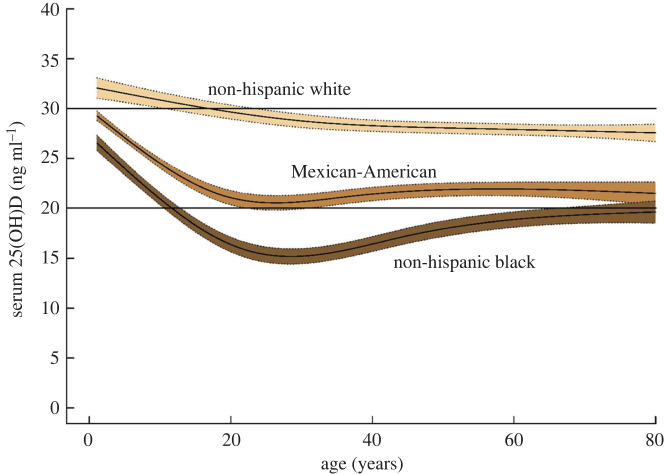
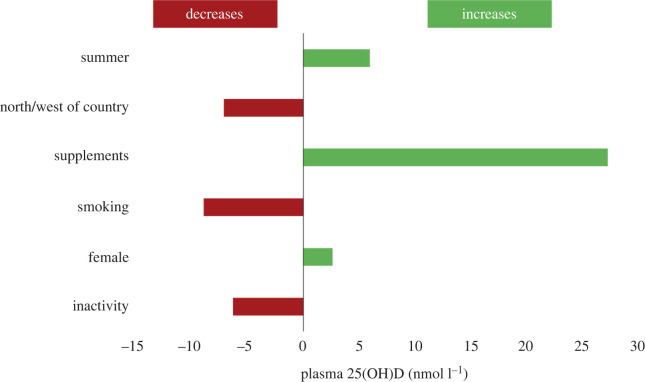
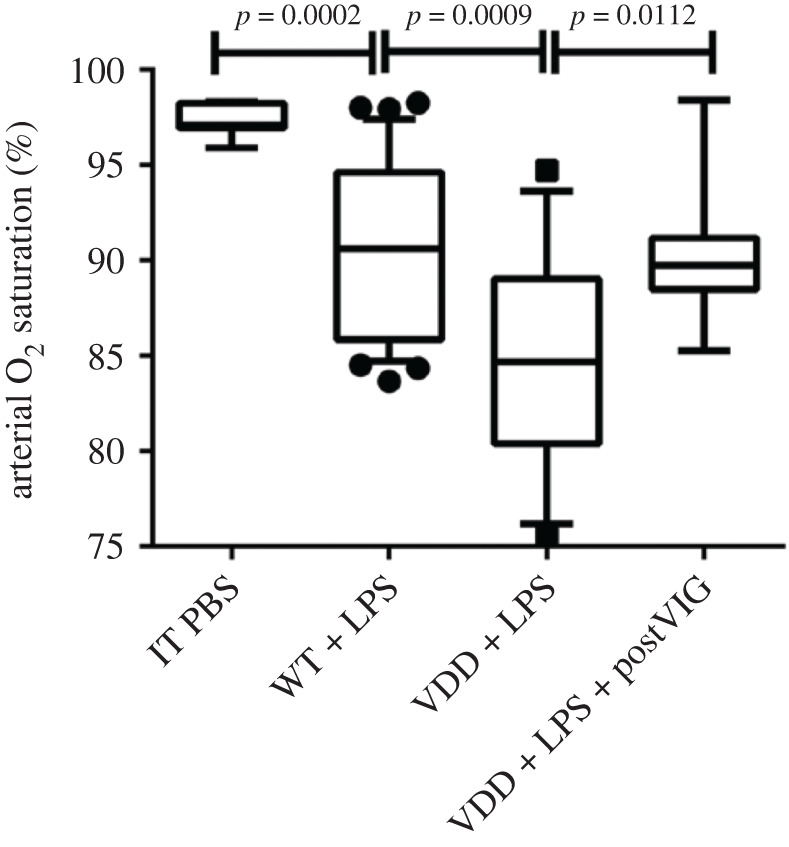
Vitamin D is a hormone that acts on many genes expressed by immune cells. Evidence linking vitamin D deficiency with COVID-19 severity is circumstantial but considerable-links with ethnicity, obesity, institutionalization; latitude and ultraviolet exposure; increased lung damage in experimental models; associations with COVID-19 severity in hospitalized patients. Vitamin D deficiency is common but readily preventable by supplementation that is very safe and cheap. A target blood level of at least 50 nmol l-1, as indicated by the US National Academy of Medicine and by the European Food Safety Authority, is supported by evidence. This would require supplementation with 800 IU/day (not 400 IU/day as currently recommended in UK) to bring most people up to target. Randomized placebo-controlled trials of vitamin D in the community are unlikely to complete until spring 2021-although we note the positive results from Spain of a randomized trial of 25-hydroxyvitamin D3 (25(OH)D3 or calcifediol) in hospitalized patients. We urge UK and other governments to recommend vitamin D supplementation at 800-1000 IU/day for all, making it clear that this is to help optimize immune health and not solely for bone and muscle health. This should be mandated for prescription in care homes, prisons and other institutions where people are likely to have been indoors for much of the summer. Adults likely to be deficient should consider taking a higher dose, e.g. 4000 IU/day for the first four weeks before reducing to 800 IU-1000 IU/day. People admitted to the hospital with COVID-19 should have their vitamin D status checked and/or supplemented and consideration should be given to testing high-dose calcifediol in the RECOVERY trial. We feel this should be pursued with great urgency. Vitamin D levels in the UK will be falling from October onwards as we head into winter. There seems nothing to lose and potentially much to gain.
Keywords: COVID-19; immunology; vitamin D.
© 2020 The Authors.
Conflict of interest statement
M.H. and D.T. have received speaking honoraria from Thornton Ross. No other competing interests.
Figures
References
LinkOut - more resources
Full Text Sources