

Diagnostic Accuracy of Endoscopic Ultrasonography Versus the Gold Standard Endoscopic Retrograde Cholangiopancreatography in Detecting Common Bile Duct Stones
- PMID: 33489574
- PMCID: PMC7813932
- DOI: 10.7759/cureus.12162
Diagnostic Accuracy of Endoscopic Ultrasonography Versus the Gold Standard Endoscopic Retrograde Cholangiopancreatography in Detecting Common Bile Duct Stones
Abstract
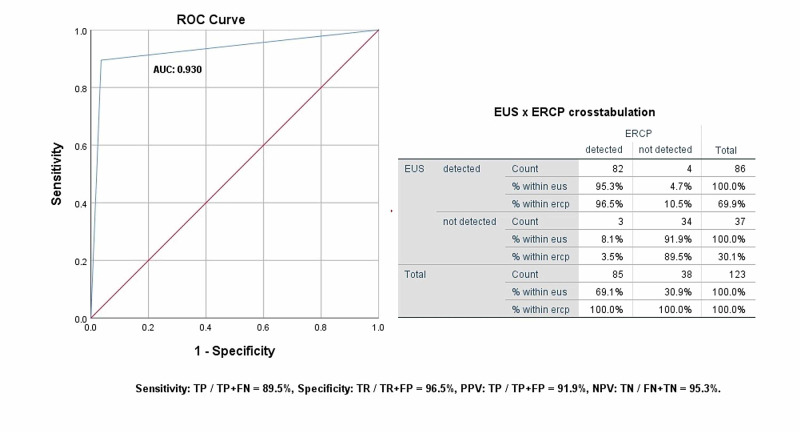
Background and objectives Stone in the biliary tract is one of the most common causes of hospitalization. However, it is difficult to determine the prevalence of gallstones in the general population because they are often asymptomatic. Thus, management lies in the proper clearance of the common bile duct (CBD) along with the removal of the gallbladder, for which it must be diagnosed on time with proper accuracy. Imaging modalities including magnetic resonance cholangiopancreatography (MRCP), endoscopic ultrasound (EUS), and endoscopic retrograde cholangiopancreatography (ERCP) provide true visualization of choledocholithiasis with comparable sensitivities. The gold standard ERCP is an invasive procedure and may cause complications, such as pancreatitis, perforation, and bleeding. EUS is a minimally invasive procedure to assess the biliary tract using high-frequency sound waves. Until now the EUS has not been addressed much in our local tertiary care setups and this study was conducted to evaluate its accuracy in the diagnosis of choledocholithiasis. The objective of our study is to determine the diagnostic accuracy (specificity and sensitivity) of EUS versus ERCP for the diagnosis of choledocholithiasis. Materials and methods This retrospective study was conducted on patients suspected of having choledocholithiasis undergoing both EUS and ERCP based on their history, clinical symptoms, and laboratory test results including upper abdominal pain, deranged liver function enzymes, and a dilated CBD on radiology. EUS was initially performed for the diagnosis of extrahepatic biliary obstruction followed by one or more of the confirmatory criterion standard tests (including ERCP). In order to reduce the chances of passage of stone resulting in negative analysis, only those patients were included in which both procedures were conducted temporally close together (24-72 hours in most instances). The main outcome measures were diagnostic accuracy with the help of sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) using a receiver operating characteristic curve. A total of 123 patients met the inclusion criteria via non-probability consecutive sampling methods. Results The mean age of our study population was 50.30 ± 13.91. We included 63 males (51.2%) and 60 females (48.8%). The most frequent indication for undergoing diagnostic procedures was deranged liver function tests (67.47%). The frequent comorbidities reported were hypertension (29.26%), diabetes (21.95%), chronic liver disease (16.26%), and ischemic heart disease (4.87%). Mean alkaline phosphatase and gamma-glutamyl transferase levels were markedly raised from the baseline in the study population. Post-ERCP complications were also reported in some of the study participants. About 85 patients (69.10%) were diagnosed with choledocholithiasis among the study participants. The diagnostic accuracy of EUS was compared with ERCP revealed an area under the curve (AUC) of 0.930, standard error of 0.031, 95% confidence interval of 0.868-0.991, the sensitivity of 89.5%, specificity of 96.5%, positive predictive value of 91.9%, and negative predictive value of 95.3%. Conclusion It is recommended that ERCP can be selectively conducted or excluded in patients with biliary obstruction in case of EUS negative, thus minimizing the complications and morbidity associated with an invasive procedure, with our results showing a comparative diagnostic accuracy of EUS.
Keywords: biliary obstruction; cbd stone; dilated common bile duct; endoscopic retrograde cholangiopancreatography (ercp); endoscopic ultrasound (eus); gastroentero-hepatology; jaundice cholestatic; receiver operating analysis; sensitivity; specificity.
Copyright © 2020, Anwer et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Diagnostic yield of endoscopic ultrasonography for dilation of common bile duct of indeterminate cause. Sousa M, Fernandes S, Proenca L, et al. Rev Esp Enferm Dig. 2019;111:757–759. - PubMed
-
- EUS for suspected choledocholithiasis: do benefits outweigh costs? A prospective, controlled study. Buscarini E, Tansini P, Vallisa D, Zambelli A, Buscarini l. Gastrointest Endosc. 2003;57:510–518. - PubMed
-
- Endosonography versus endoscopic retrograde cholangiopancreatography in diagnosing extrahepatic biliary obstruction. Angelo TDI, Prochazka V, Holinka M, et al. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2011;155:339–346. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous