

Multiple Brown tumors in a Case of Primary Hyperparathyroidism with Pathological Fracture in Femur
- PMID: 33489969
- PMCID: PMC7815671
- DOI: 10.13107/jocr.2020.v10.i06.1872
Multiple Brown tumors in a Case of Primary Hyperparathyroidism with Pathological Fracture in Femur
Abstract
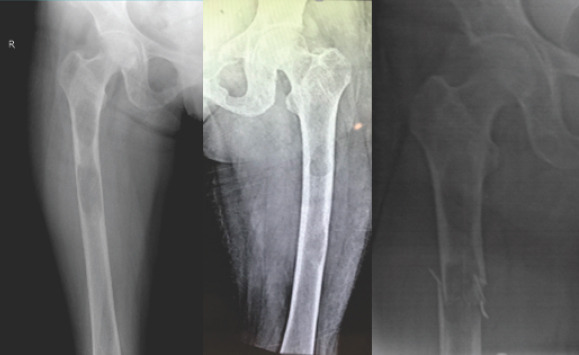
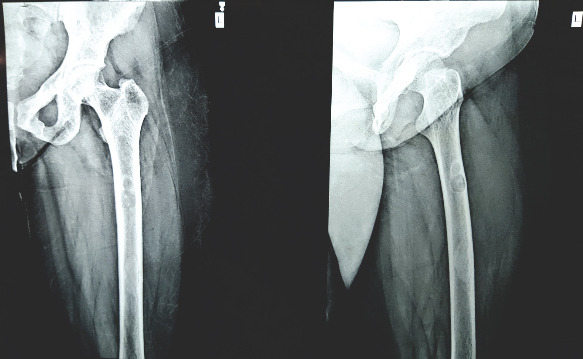
Introduction: Pathological fractures in long bones are commonly caused by simple bone cyst or Osteogenesis imperfecta in children and by metastatic tumors from primary carcinoma, multiple myeloma, osteoporosis, and bone tumors in adults. Hyperparathyroidism causing pathological fractures, though a well-known entity, is seen infrequently in clinical practice. The fractures occur in the expansile fibro-cystic bone lesions called as "Brown tumor." The reported case describes a patient with classical features of primary hyperparathyroidism (PHPT) having multiple lytic lesions in pelvis and bilateral femur with pathological fracture. It is being reported due to its rarity.
Case report: A 28-year-old young married lady presented with chronic dull aching pain in both thighs and difficulty in walking for 2 years. Examination revealed tenderness in both thighs, with antalgic gait. X-ray pelvis with both thighs showed multiple lytic lesions of variable size in both femora and pelvis. Blood investigations showed raised levels of serum calcium, with highly raised levels of serum parathyroid hormone (PTH). Contrast-enhanced computerized tomography (CT) scan of neck demonstrated parathyroid adenoma. The patient admitted for prophylactic nailing for right femur, developed a fracture while indoor and was managed by right proximal femoral nailing, followed by parathyroid adenoma excision. Follow-up showed dramatic clinical and radiological improvement with good healing of fracture. Lytic lesions healed gradually and blood parameters returned to normal. The patient remains asymptomatic at 2 years follow-up.
Conclusion: Advanced case of symptomatic PHPT affecting bones is rare and it should be considered as a differential diagnosis in cases of a solitary and or multiple osteolytic lesions. Serum calcium and PTH level estimation at an early stage prevents missing the diagnosis and progression of disease. Early diagnosis and appropriate treatment help in rapid clinical improvement with almost total reversal of bony changes, thus avoiding devastating complications.
Keywords: Hyperparathyroidism; brown tumor; femur; osteitis fibrosa cystica; pathological fracture.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: Nil
Figures




References
-
- Jain AK, Jajodia N. Metabolic bone diseases and related dysfunction of the parathyroid glands. In: Jain AK, editor. Turek's Orthopaedics. 7th ed. South Holland, Netherlands: Wolters Kluwer; 2017. pp. 251–6.
-
- Hong WS, Sung MS, Chun KA, Kim JY, Park SW, Lee KH, et al. Emphasis on the MR imaging findings of brown tumor: A report of five cases. Skeletal Radiol. 2011;40:205–13. - PubMed
-
- Eller-Vainicher C, Filopanti M, Palmieri S, Ulivieri FM, Morelli V, Zhukouskaya VV, et al. Bone quality, as measured by trabecular bone score, in patients with primary hyperparathyroidism. Eur J Endocrinol. 2013;169:155–62. - PubMed
Publication types
LinkOut - more resources
Full Text Sources