

Nonanatomical Reduction of Femoral Neck Fractures in Young Patients (≤65 Years Old) with Internal Fixation Using Three Parallel Cannulated Screws
- PMID: 33490267
- PMCID: PMC7801101
- DOI: 10.1155/2021/3069129
Nonanatomical Reduction of Femoral Neck Fractures in Young Patients (≤65 Years Old) with Internal Fixation Using Three Parallel Cannulated Screws
Abstract
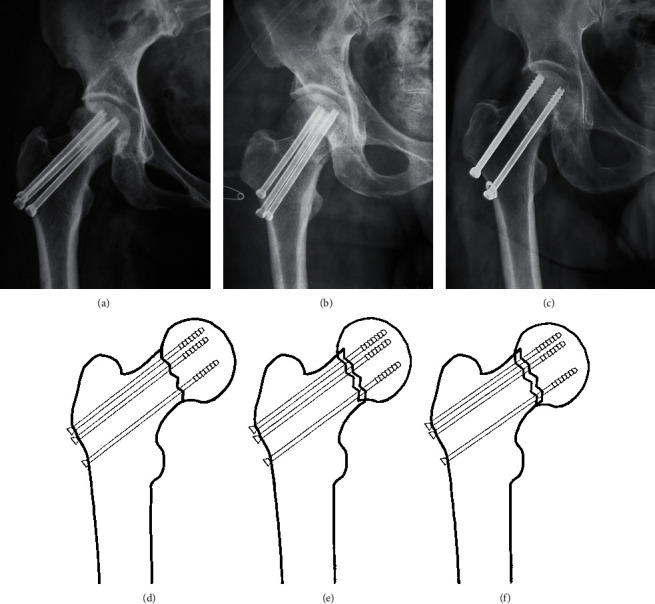
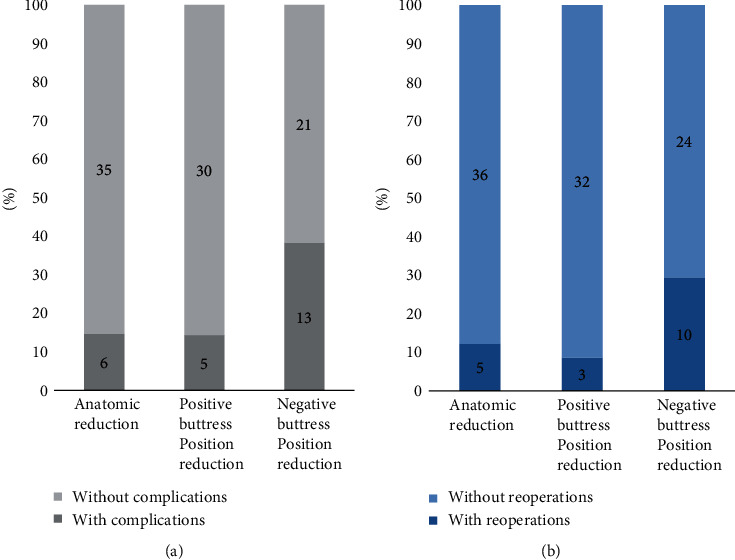
Purpose: The study is aimed at investigating the association between different reduction classifications (anatomic reduction, positive buttress position reduction, and negative buttress position reduction) and two end points (complications and reoperations).
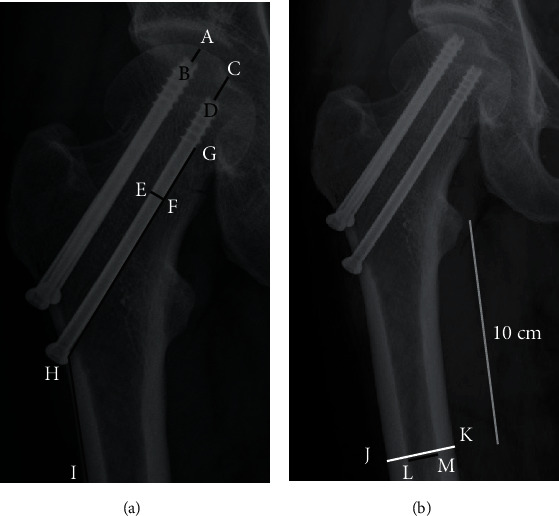
Methods: The study retrospectively analyzed 110 patients undergoing internal fixation with three parallel cannulated screws from January 2012 to January 2019 in Huashan Hospital. Based on the principles of the "Gotfried reduction," all enrolled patients were divided into three groups: anatomic reduction, positive buttress position reduction, and negative buttress position reduction intraoperatively or immediately after surgery. Clinical characteristics including age, sex, side, Garden classification, Pauwels classification, fracture level, reduction classification, Garden alignment index angles, cortical thickness index (CTI), tip-caput distance (TCD), angle of the inferior screw, and the two ending points (complications and reoperations) were included in the statistical analysis. The Mann-Whitney U-test, the chi-square test, Fisher's exact test, and multiple logistic regression analysis were used in the study.
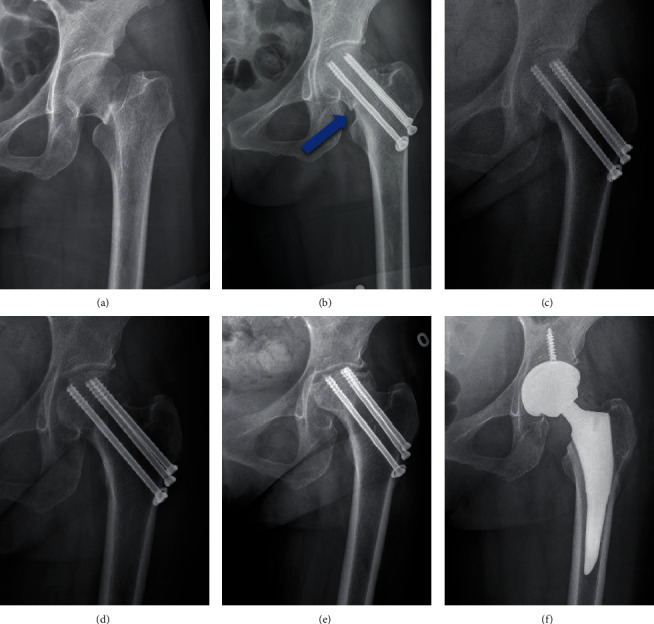
Results: Of the 110 patients included in our study, the mean ± standard deviation (SD) of age was 51.4 ± 10.4 years; 41 patients showed anatomic reduction, 35 patients showed positive buttress position reduction, and 34 patients showed negative buttress position reduction. For the outcomes, 24 patients (anatomic reduction: 6 [14.6%]; positive buttress position reduction: 5 [14.3%]; negative buttress position reduction: 13 [38.2%]) had complications, while 18 patients (anatomic reduction: 5 [12.2%]; positive buttress position reduction: 3 [8.6%]; negative buttress position reduction: 10 [29.4%]) underwent reoperations after surgery. In the multivariate logistic regression analysis of complications, negative buttress position reduction (negative buttress position reduction vs. anatomic reduction, OR = 4.309, 95%CI = 1.137 to 16.322, and p = 0.032) was found to be correlated with higher risk of complications. The same variable (negative buttress position reduction vs. anatomic reduction, OR = 5.744, 95%CI = 1.177 to 28.042, and p = 0.031) was also identified as risk factor in the multivariate logistic regression analysis of reoperations. However, no significant difference between positive reduction and anatomical reduction was investigated in the analysis of risk factors for complications, not reoperations.
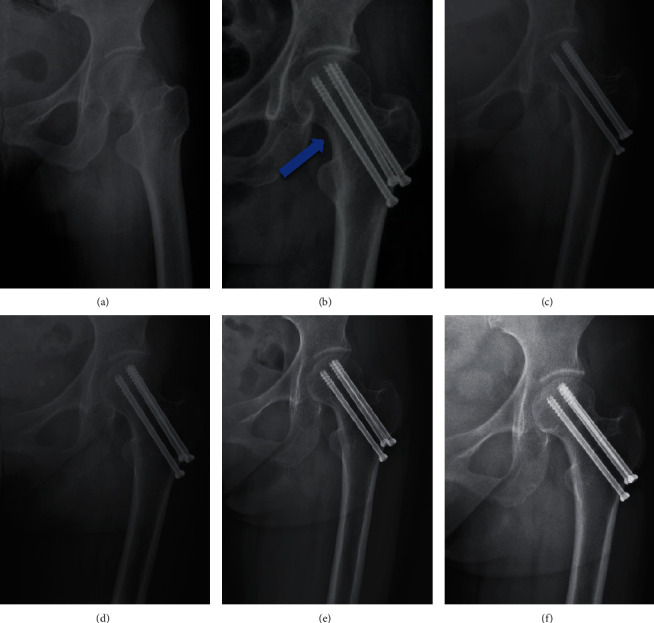
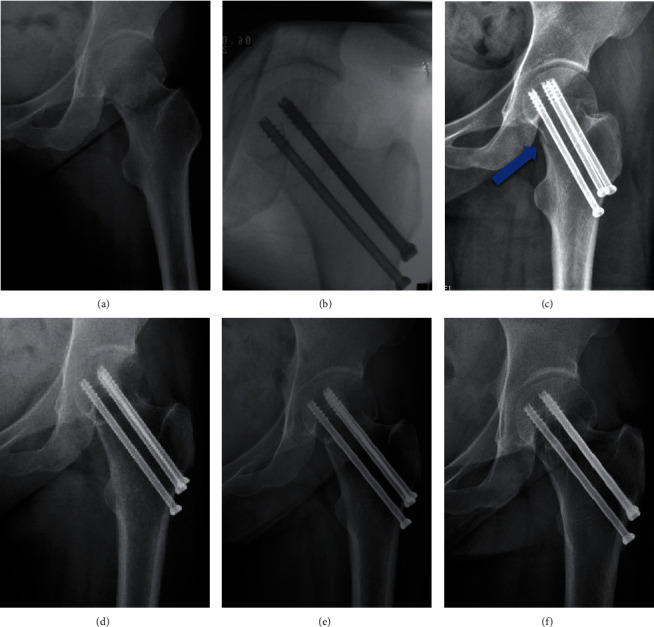
Conclusion: Positive buttress position reduction of femoral neck fractures in young patients showed a similar incidence of complications and reoperations compared with those of anatomic reduction. For irreversible femoral neck fractures, if positive buttress position reduction has been achieved intraoperatively, it is not necessary to pursue anatomical reduction; however, negative reduction needs to be avoided.
Copyright © 2021 Guanglei Zhao et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Biz C., Tagliapietra J., Zonta F., Belluzzi E., Bragazzi N. L., Ruggieri P. Predictors of early failure of the cannulated screw system in patients, 65 years and older, with non-displaced femoral neck fractures. Aging Clinical and Experimental Research. 2020;32(3):505–513. doi: 10.1007/s40520-019-01394-1. - DOI - PubMed
-
- Ly T. V., Swiontkowski M. F. Treatment of femoral neck fractures in young adults. Journal of Bone and Joint Surgery. 2008;90(10):2254–2266. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
