

The Discriminant Use of Intrauterine Balloon Tamponade and Compression Sutures for Management of Major Postpartum Hemorrhage: Comparison of Patient Characteristics and Clinical Outcome
- PMID: 33490275
- PMCID: PMC7801069
- DOI: 10.1155/2021/6648829
The Discriminant Use of Intrauterine Balloon Tamponade and Compression Sutures for Management of Major Postpartum Hemorrhage: Comparison of Patient Characteristics and Clinical Outcome
Abstract
Background: Intrauterine balloon tamponade (IUBT) and compression sutures have been widely used in recent years in the management of postpartum hemorrhage (PPH). However, there is scant literature directly comparing the clinical scenarios that led to the discriminant selection of these management modalities and the direct clinical outcomes. The purpose of this study is to compare the patient characteristics and clinical risk factors that led to the use of IUBT and compression sutures in the management of major PPH as well as the immediate outcome in a retrospective cohort.
Methods: Patients who had IUBT or compression sutures applied due to major PPH (>1000 ml) from 2014 to 2018 in a single obstetric unit were recruited. The patient characteristics and clinical outcome of the two groups were compared.
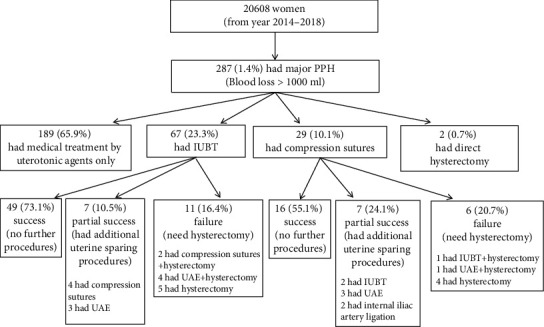
Results: A total of 67 patients had IUBT and 29 patients had compression sutures applied as the first uterine sparing technique. Apart from more vaginal deliveries (25.4% vs. 3.5%) in the IUBT group compared to compression sutures, there were no significant differences between the two groups in terms of patient characteristics. The IUBT group had a slightly higher blood loss at the start of the uterine sparing procedure (239 ml, p = 0.049) and received more transfusions, despite no differences in the total blood loss, hemogloblin level, incidence of coagulopathy, and intensive care unit admission between the two groups. There was no significant difference in the overall success rate between IUBT and compression sutures to control PPH without additional surgical intervention or hysterectomy (73.1% vs. 55.1%, p = 0.15) or the success rate for PPH due to uterine atony (32.8% vs. 20.7%), though IUBT apparently performed better than compression sutures in cases of placenta praevia (77.3% vs. 16.7%, p = 0.01). Blood loss > 1.5 l at the start of the procedure, presence of placenta accreta, and presence of coagulopathy were found to be significant poor prognostic factors for both procedures to control PPH.
Conclusions: There were no dominating patient characteristics that favoured the selection of either IUBT or compression sutures in the management of severe PPH except for the mode of delivery. Both procedures had equally high overall success rates to control PPH, but IUBT performed better in placenta praevia cases as compared to compression sutures.
Copyright © 2021 Choi Wah Kong and William Wing Kee To.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this article.
Figures
Similar articles
-
Prognostic factors for the use of intrauterine balloon tamponade in the management of severe postpartum hemorrhage.Int J Gynaecol Obstet. 2018 Jul;142(1):48-53. doi: 10.1002/ijgo.12498. Epub 2018 Apr 17. Int J Gynaecol Obstet. 2018. PMID: 29603742
-
Intrauterine balloon tamponade for management of severe postpartum haemorrhage in a perinatal network: a prospective cohort study.BJOG. 2017 Jul;124(8):1255-1262. doi: 10.1111/1471-0528.14382. Epub 2016 Oct 25. BJOG. 2017. PMID: 27781401
-
Predictors of failed intrauterine balloon tamponade for persistent postpartum hemorrhage after vaginal delivery.PLoS One. 2018 Oct 26;13(10):e0206663. doi: 10.1371/journal.pone.0206663. eCollection 2018. PLoS One. 2018. PMID: 30365539 Free PMC article.
-
Intrauterine balloon tamponade in the management of severe postpartum haemorrhage after vaginal delivery: Is the failure early predictable?Eur J Obstet Gynecol Reprod Biol. 2021 Mar;258:317-323. doi: 10.1016/j.ejogrb.2021.01.030. Epub 2021 Jan 20. Eur J Obstet Gynecol Reprod Biol. 2021. PMID: 33498006 Review.
-
Novel concepts and improvisation for treating postpartum haemorrhage: a narrative review of emerging techniques.Reprod Health. 2023 Aug 11;20(1):116. doi: 10.1186/s12978-023-01657-1. Reprod Health. 2023. PMID: 37568196 Free PMC article. Review.
Cited by
-
Obstetric and Maternal Outcomes After B-Lynch Compression Sutures: A Meta-Analysis.Cureus. 2022 Nov 9;14(11):e31306. doi: 10.7759/cureus.31306. eCollection 2022 Nov. Cureus. 2022. PMID: 36514660 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
