

Hiding in plain sight: Gene panel and genetic markers reveal 26-year undiagnosed tumor-induced osteomalacia of the rib concurrently misdiagnosed as X-linked hypophosphatemia
- PMID: 33490314
- PMCID: PMC7804981
- DOI: 10.1016/j.bonr.2020.100744
Hiding in plain sight: Gene panel and genetic markers reveal 26-year undiagnosed tumor-induced osteomalacia of the rib concurrently misdiagnosed as X-linked hypophosphatemia
Abstract
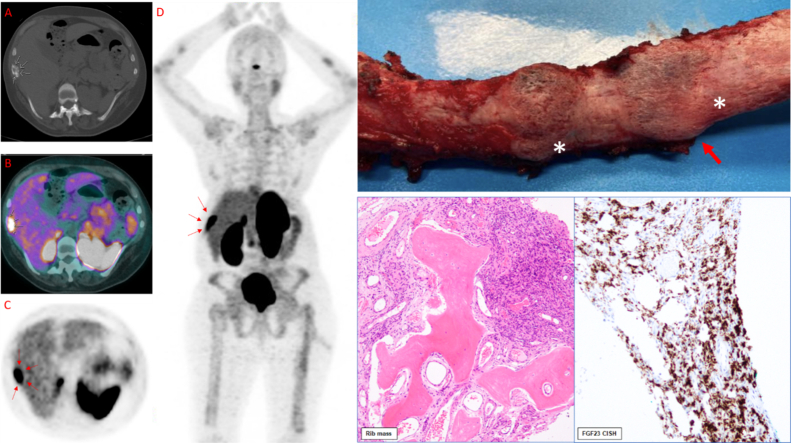
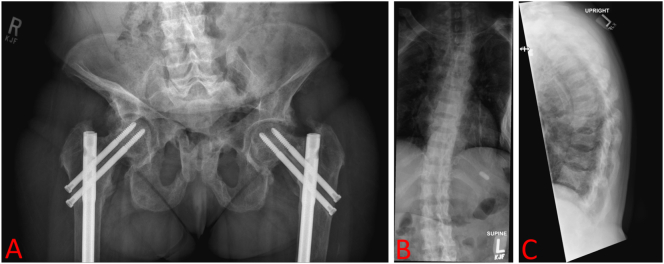
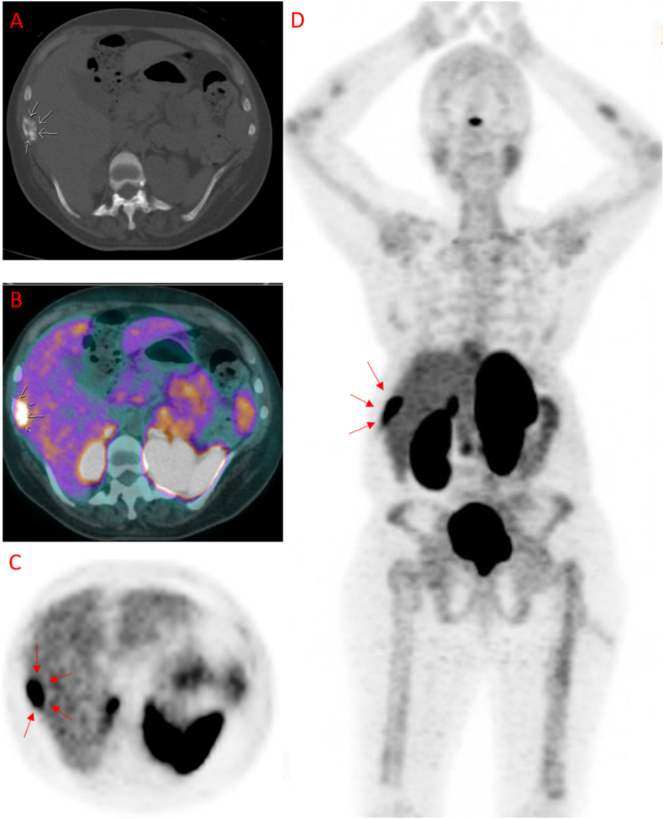
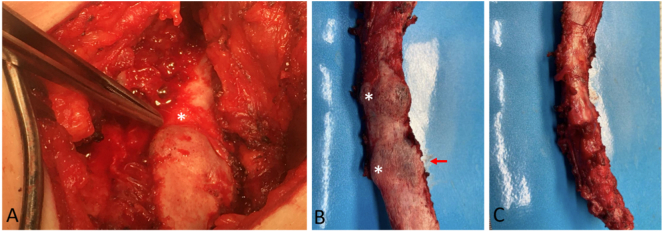
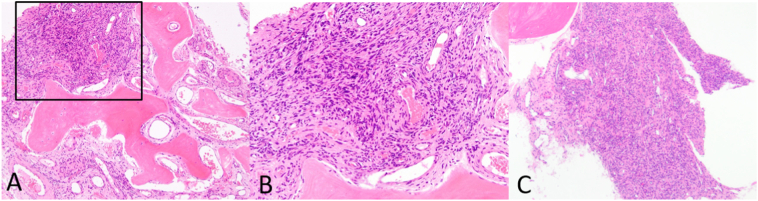
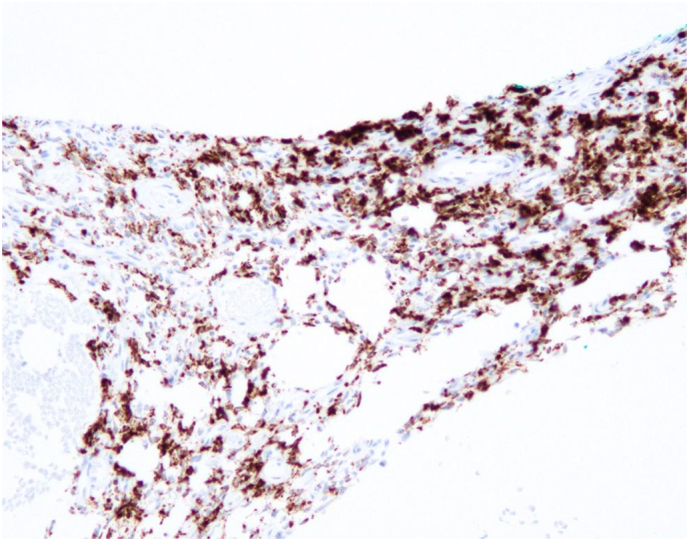
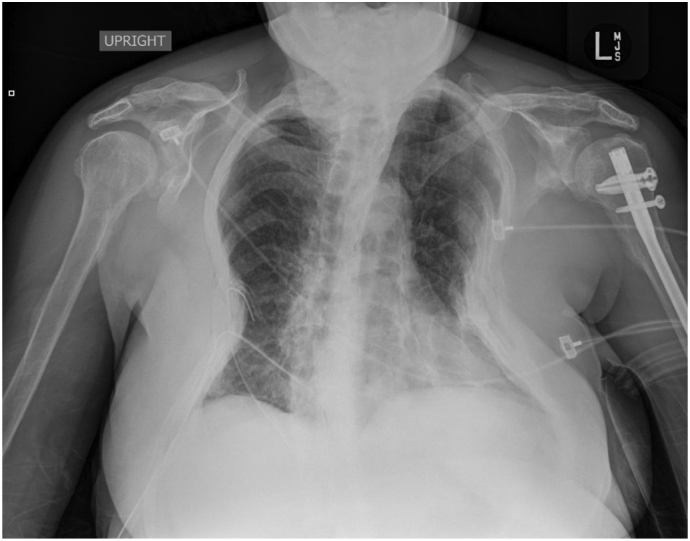
Tumor-induced osteomalacia (TIO), caused by phosphaturic mesenchymal tumors (PMTs), is a rare paraneoplastic syndrome characterized by frequent bone fractures, bone pain, muscle weakness, and affected gait. These tumors typically secrete high levels of Fibroblastic Growth Factor 23 (FGF23), a hormone which acts on the kidney to cause hypophosphatemia, ultimately impairing bone mineralization. In this case report, we present a 41-year-old female with FGF23-mediated hypophosphatemia with a 26-year delay in TIO diagnosis and a concurrent misdiagnosis of X-linked hypophosphatemic rickets (XLH). Given an absence of family history of hypophosphatemia, a 13-gene hypophosphatemia panel including XLH (PHEX gene) was performed and came back negative prompting a diagnostic search for a PMT causing TIO. A 68Ga-DOTATATE PET/CT scan revealed the presence of a 9th right rib lesion, for which she underwent rib resection. The patient's laboratory values (notably serum phosphorus, calcium, and vitamin D) normalized, with FGF23 decreasing immediately after surgery, and symptoms resolving over the next three months. Chromogenic in situ hybridization (CISH) and RNA-sequencing of the tumor were positive for FGF23 (CISH) and the transcriptional marker FN1-FGFR1, a novel fusion gene between fibronectin (FN1) and Fibroblast Growth Factor Receptor 1 (FGFR1), previously determined to be present in the majority of TIO-associated tumors. This case demonstrates the notion that rare and diagnostically challenging disorders like TIO can be undiagnosed and/or misdiagnosed for many years, even by experienced clinicians and routine lab testing. It also underscores the power of novel tools available to clinicians such as gene panels, CISH, and RNA sequencing, and their ability to characterize TIO and its related tumors in the context of several phenotypically similar diseases.
Keywords: 68Ga-DOTATATE; Burosumab; Chromogenic in situ hybridization; FGF23; FGFR1; FN1; FN1-FGFR1; Fibroblast growth factor 23; Fibroblast growth factor receptor 1; PHEX; Paraneoplastic; Phosphaturic mesenchymal tumor; RNA sequencing; TIO; Tumor-induced osteomalacia; X-linked hypophosphatemic rickets; XLH; fibronectin; phosphate wasting disorders; phosphorous.
© 2020 The Authors.
Figures
References
-
- Carpenter T.O. New perspectives on the biology and treatment of X-linked hypophosphatemic rickets. Pediatr. Clin. N. Am. 1997;44:443–466. - PubMed
-
- M. P. Carpenter T.O., Weber T., Peacock M., Ruppe M., Insogna K., Osei S., Luca D., Skrinar A., San Martin J. (2016) Effects of KRN23, and anti-FGF23 antibody, in patients with tumor induced osteomalacia and epidermal nevus syndrome: results from an ongoing phase 2 study. in Jan De Beur S. Annual Meeting of the American Society for Bone and Mineral Research 1098.
-
- Carter J.M., Caron B.L., Dogan A., Folpe A.L. A novel chromogenic in situ hybridization assay for FGF23 mRNA in phosphaturic mesenchymal tumors. Am. J. Surg. Pathol. 2015;39:75–83. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
