

Characterization of one anastomosis gastric bypass and impact of biliary and common limbs on bile acid and postprandial glucose metabolism in a minipig model
- PMID: 33491532
- PMCID: PMC8906817
- DOI: 10.1152/ajpendo.00356.2020
Characterization of one anastomosis gastric bypass and impact of biliary and common limbs on bile acid and postprandial glucose metabolism in a minipig model
Abstract
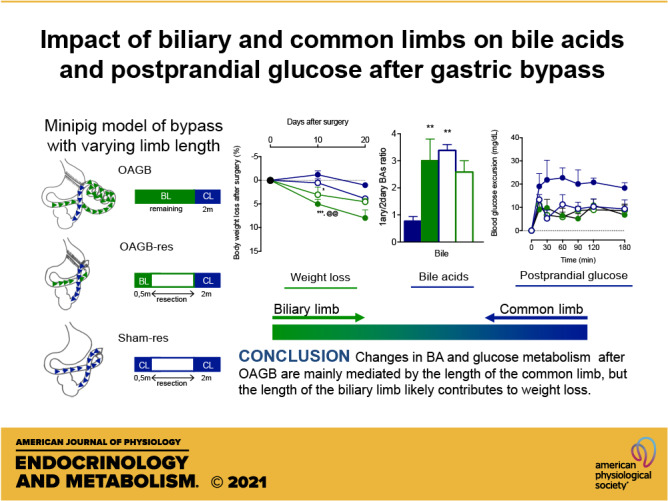
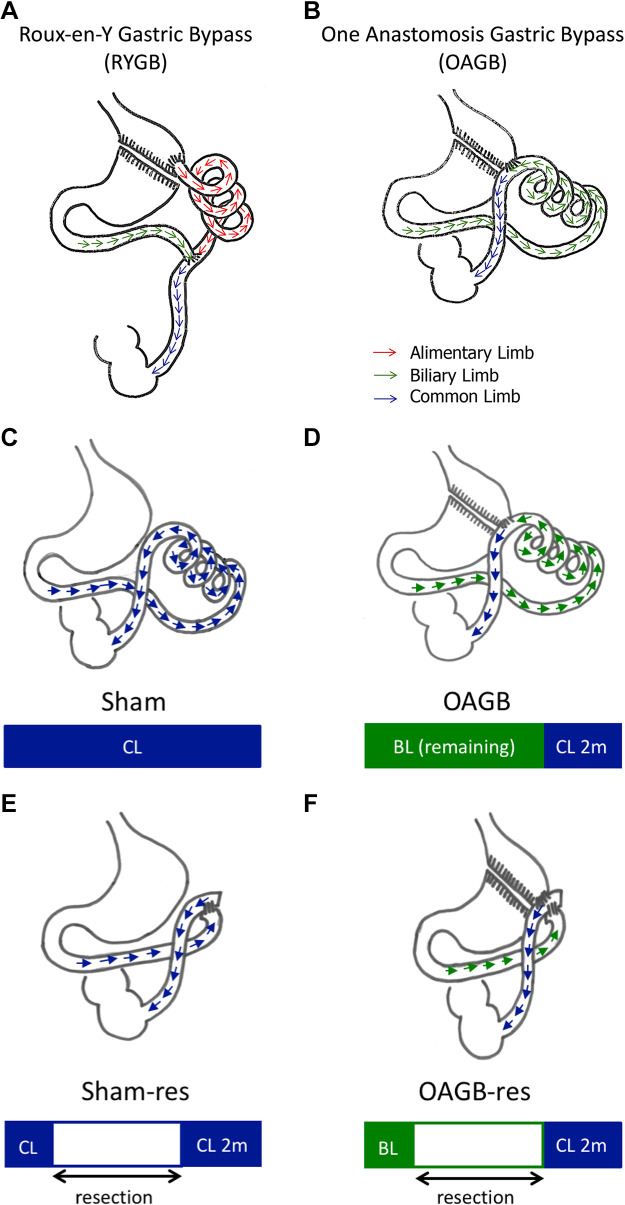
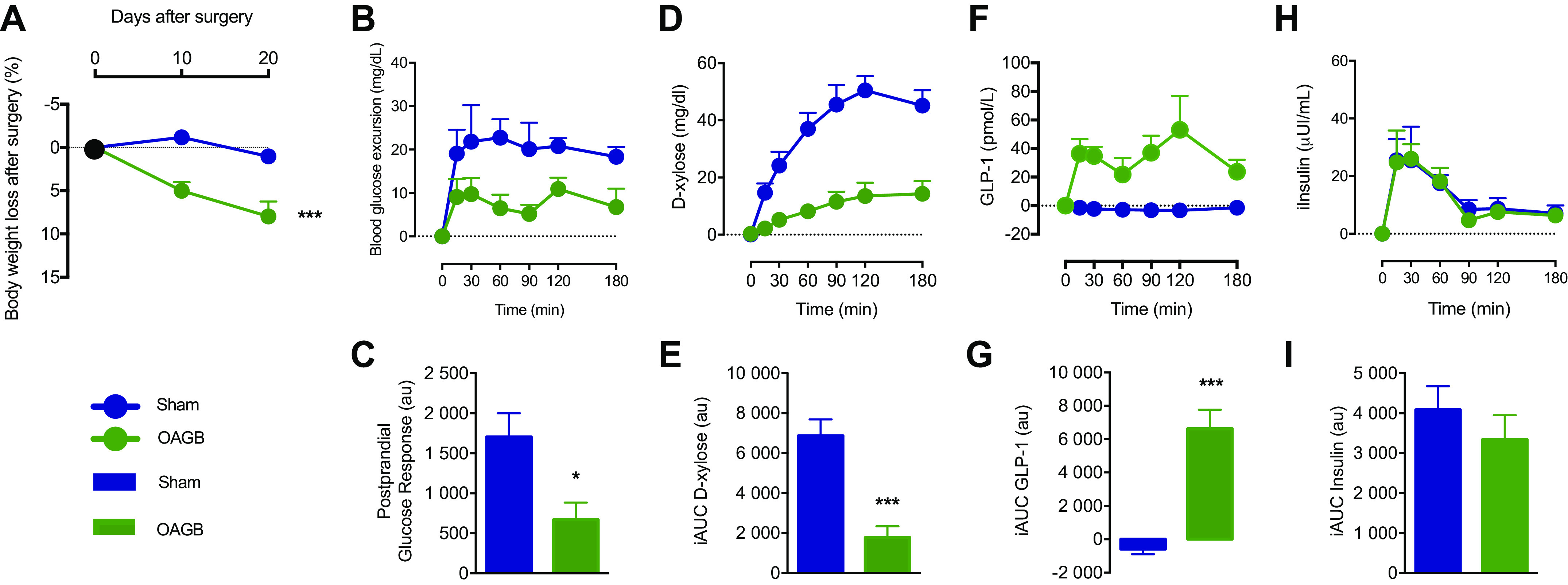
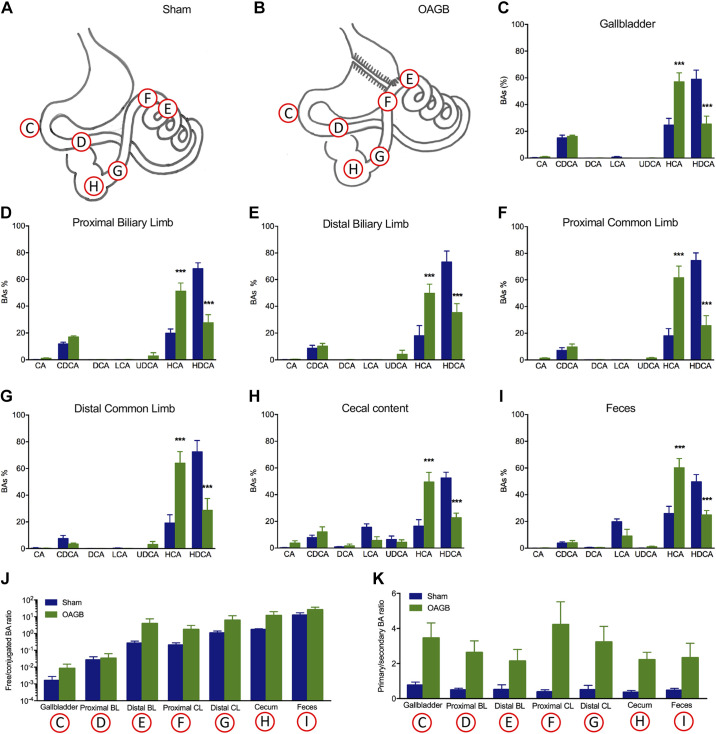
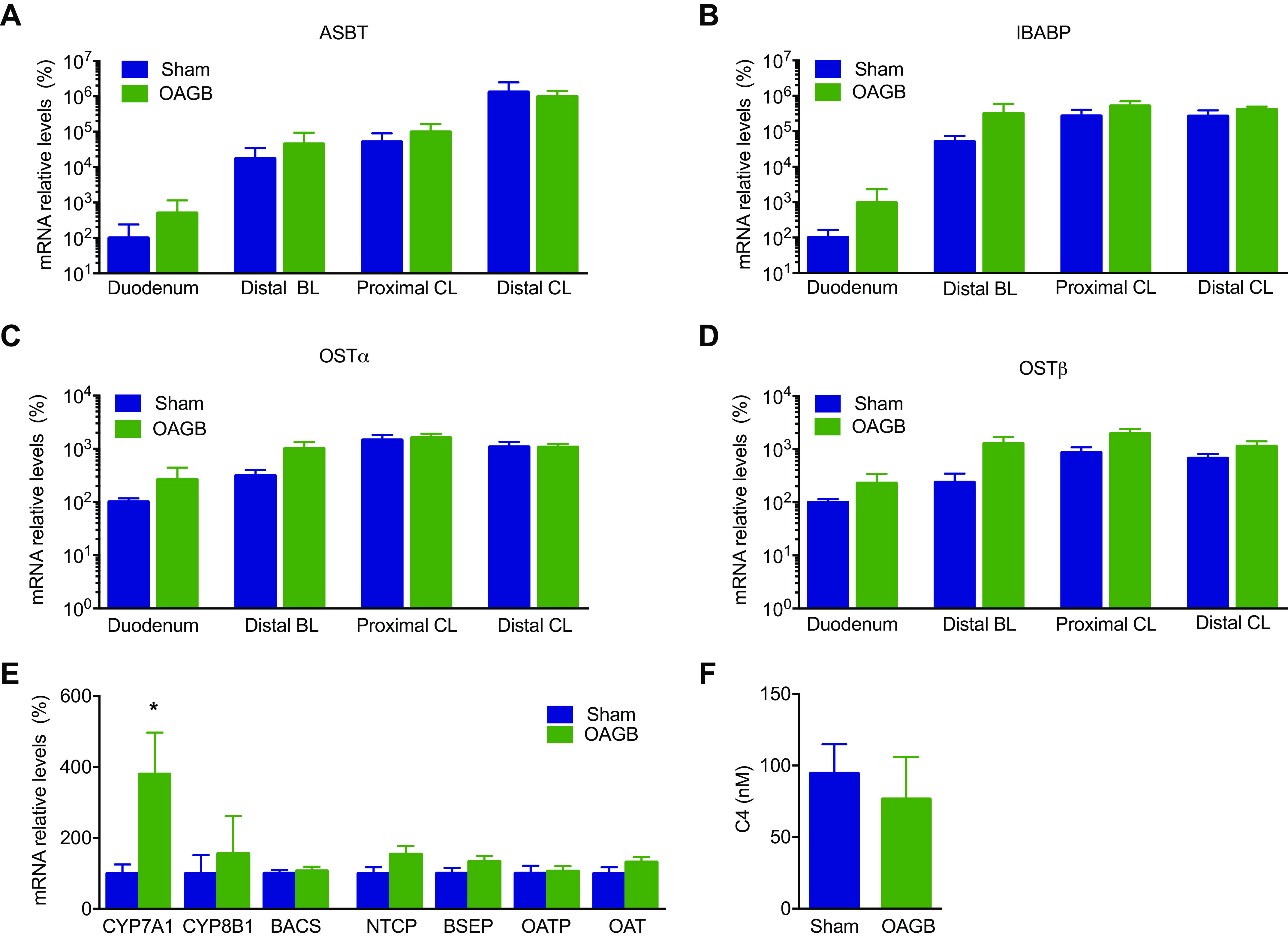
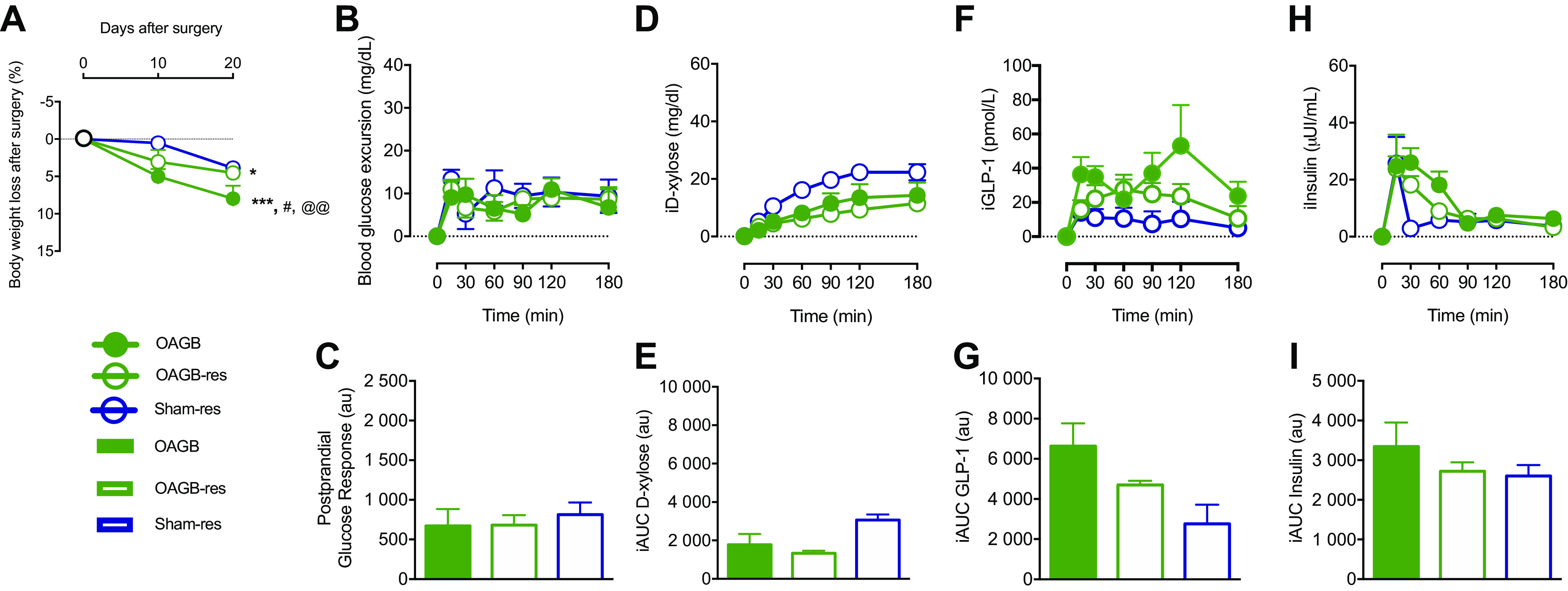
The alimentary limb has been proposed to be a key driver of the weight-loss-independent metabolic improvements that occur upon bariatric surgery. However, the one anastomosis gastric bypass (OAGB) procedure, consisting of one long biliary limb and a short common limb, induces similar beneficial metabolic effects compared to Roux-en-Y Gastric Bypass (RYGB) in humans, despite the lack of an alimentary limb. The aim of this study was to assess the role of the length of biliary and common limbs in the weight loss and metabolic effects that occur upon OAGB. OAGB and sham surgery, with or without modifications of the length of either the biliary limb or the common limb, were performed in Gottingen minipigs. Weight loss, metabolic changes, and the effects on plasma and intestinal bile acids (BAs) were assessed 15 days after surgery. OAGB significantly decreased body weight, improved glucose homeostasis, increased postprandial GLP-1 and fasting plasma BAs, and qualitatively changed the intestinal BA species composition. Resection of the biliary limb prevented the body weight loss effects of OAGB and attenuated the postprandial GLP-1 increase. Improvements in glucose homeostasis along with changes in plasma and intestinal BAs occurred after OAGB regardless of the biliary limb length. Resection of only the common limb reproduced the glucose homeostasis effects and the changes in intestinal BAs. Our results suggest that the changes in glucose metabolism and BAs after OAGB are mainly mediated by the length of the common limb, whereas the length of the biliary limb contributes to body weight loss.NEW & NOTEWORTHY Common limb mediates postprandial glucose metabolism change after gastric bypass whereas biliary limb contributes to weight loss.
Keywords: bariatric; bariatric surgery; bile acids; biliary limb; bypass; common limb; one anastomosis gastric bypass.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures

References
-
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, Mullany EC, et al. . Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 384: 766–781, 2014. doi:10.1016/S0140-6736(14)60460-8. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials