

The Pathology of the Vestibular System in CANVAS
- PMID: 33492056
- PMCID: PMC9234914
- DOI: 10.1097/MAO.0000000000002985
The Pathology of the Vestibular System in CANVAS
Abstract
Objective: To describe the site of lesion responsible for the severe, bilateral, symmetrical, selective loss of vestibular function in Cerebellar Ataxia with Neuronopathy and Vestibular Areflexia Syndrome (CANVAS), an adult-onset recessively-inherited ataxia, characterized by progressive imbalance due to a combination of cerebellar, somatosensory, and selective vestibular impairment with normal hearing.
Methods: Histologic examination of five temporal bones and the brainstems from four CANVAS patients and the brainstem only from one more, each diagnosed and followed from diagnosis to death by one of the clinician authors.
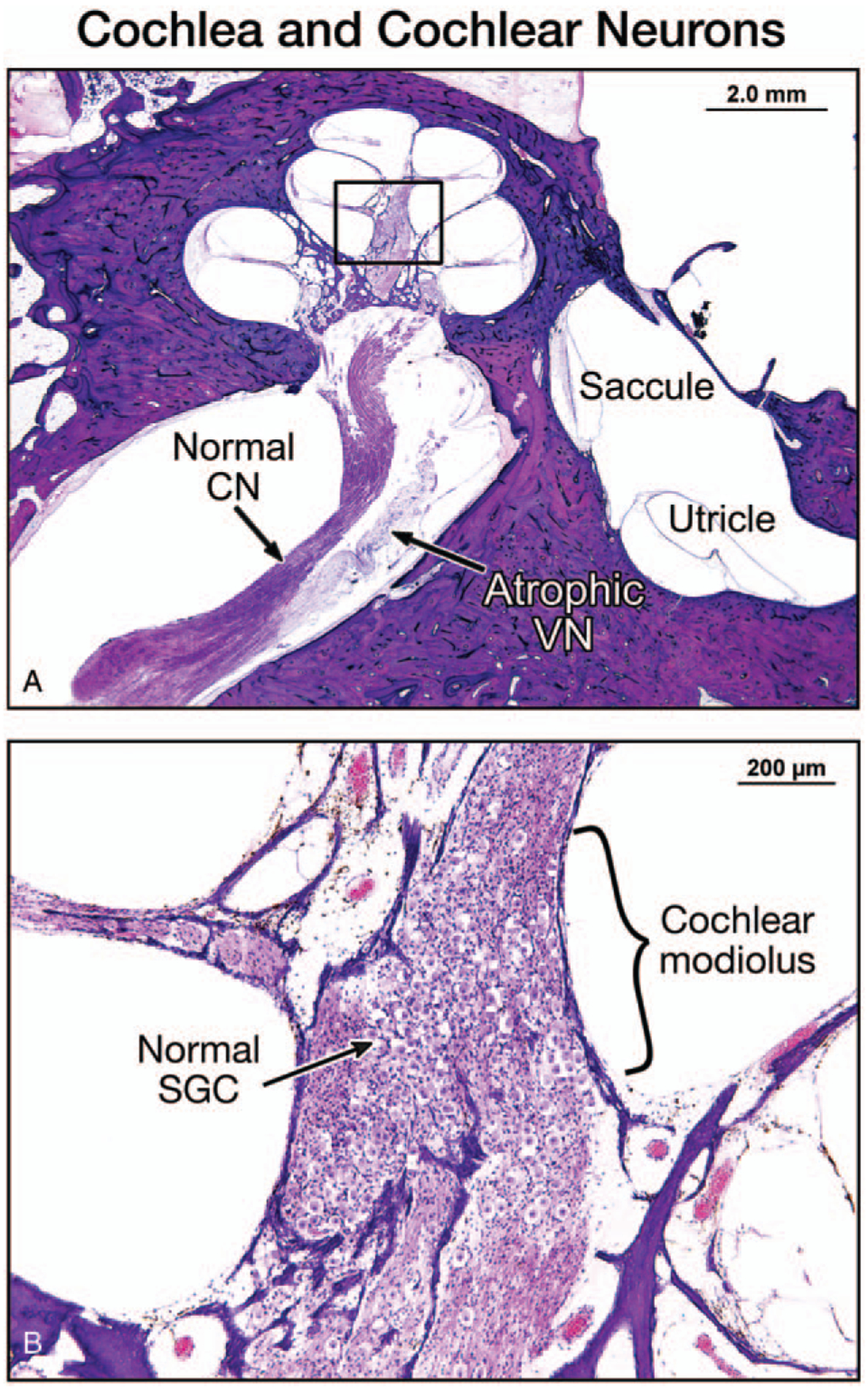
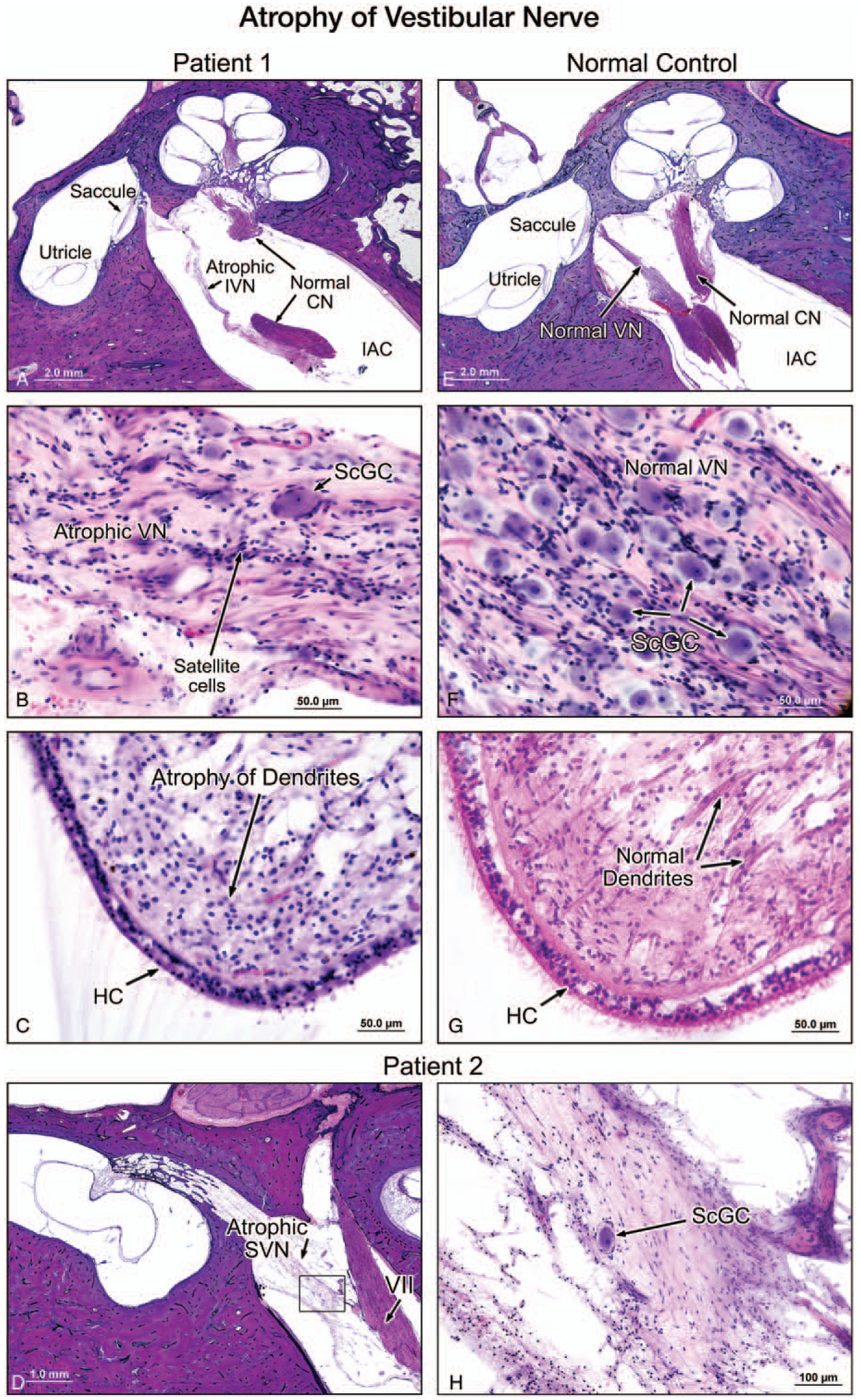
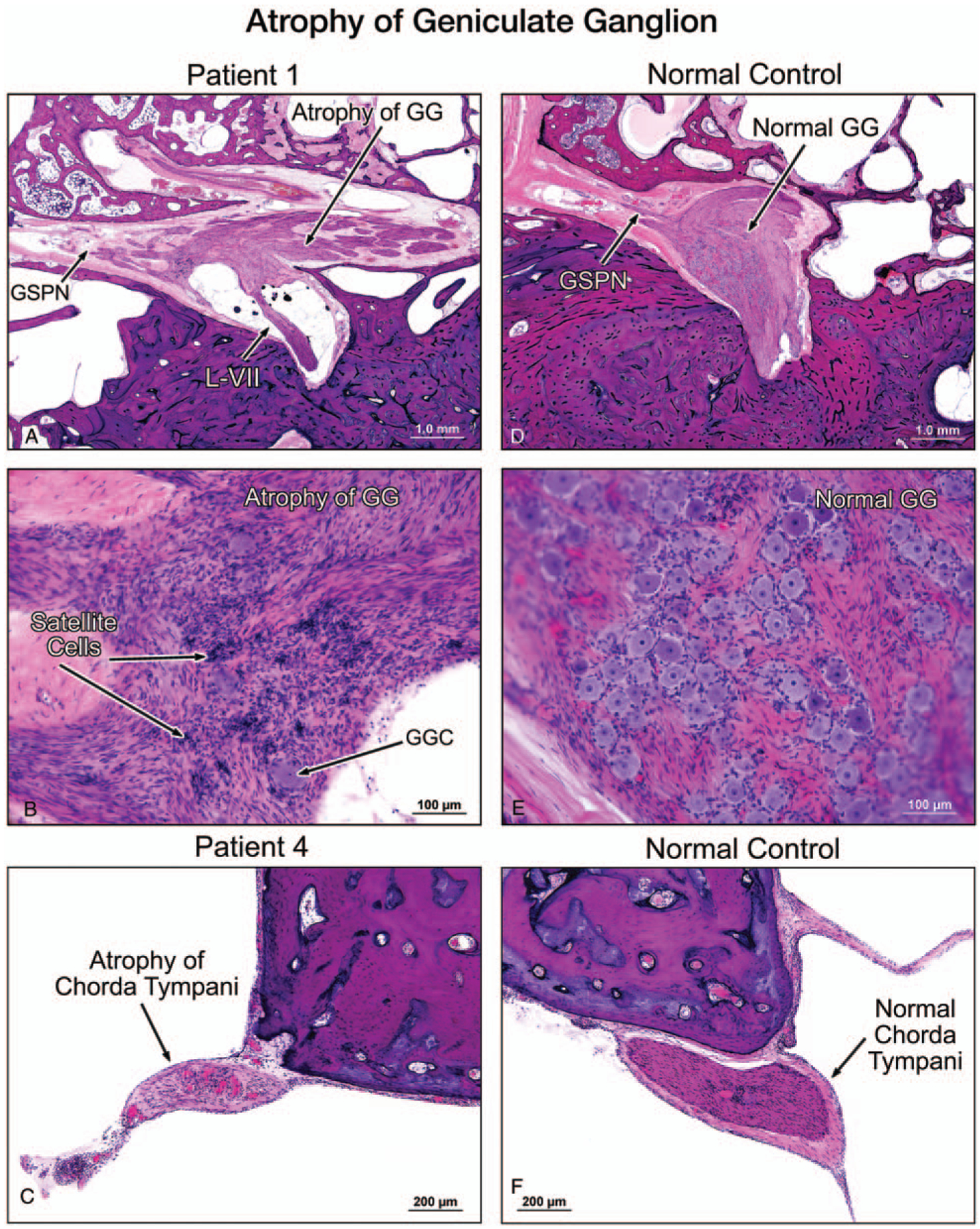
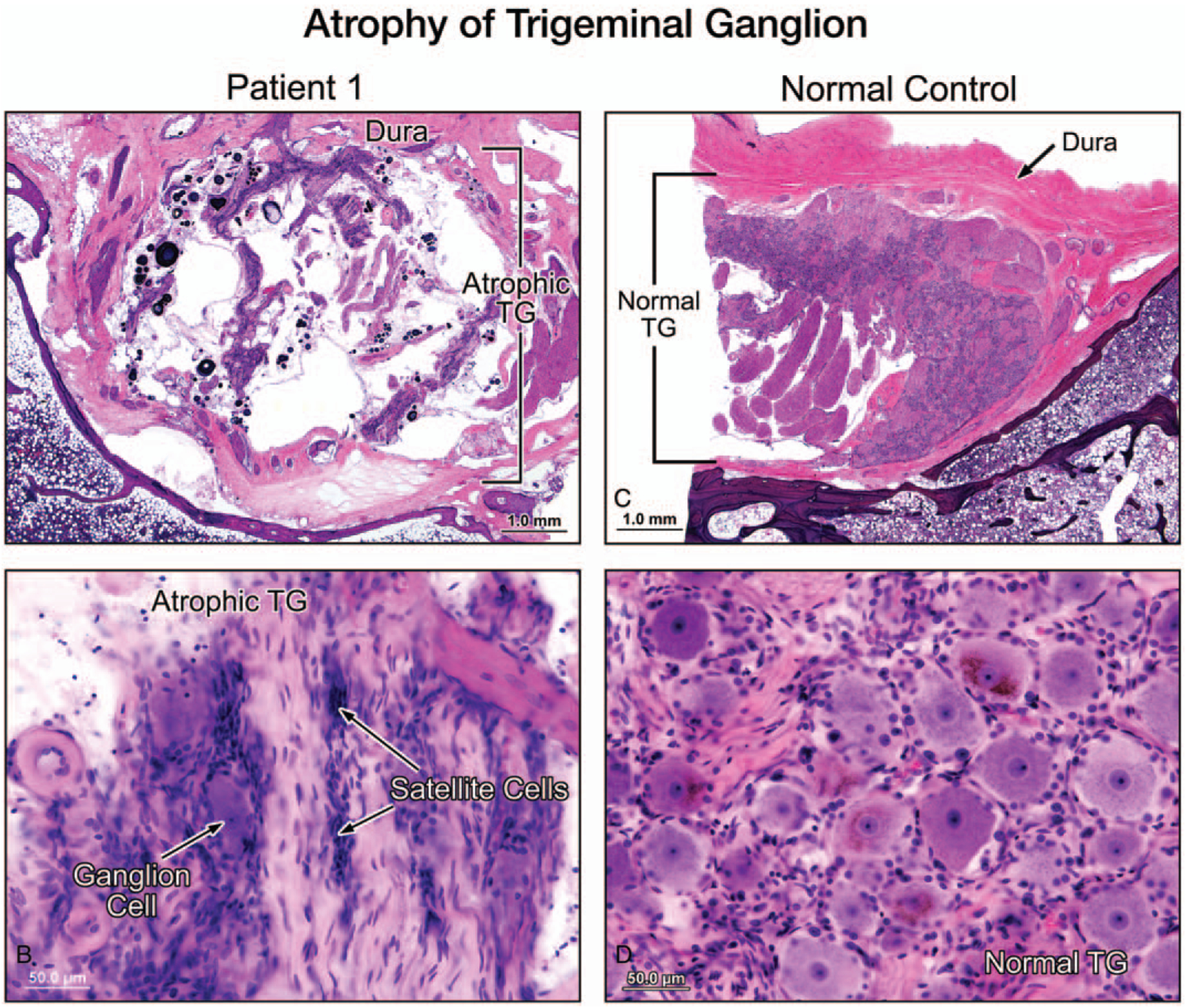
Results: All five temporal bones showed severe loss of vestibular ganglion cells (cell counts 3-16% of normal), and atrophy of the vestibular nerves, whereas vestibular receptor hair cells and the vestibular nuclei were preserved. In contrast, auditory receptor hair cells, the auditory ganglia (cell counts 51-100% of normal), and the auditory nerves were relatively preserved. In addition, the cranial sensory ganglia (geniculate and trigeminal), present in two temporal bones, also showed severe degeneration.
Conclusions: In CANVAS there is a severe cranial sensory ganglionopathy neuronopathy (ganglionopathy) involving the vestibular, facial, and trigeminal ganglia but sparing the auditory ganglia. These observations, when coupled with the known spinal dorsal root ganglionopathy in CANVAS, indicate a shared pathogenesis of its somatosensory and cranial nerve manifestations. This is the first published account of both the otopathology and neuropathology of CANVAS, a disease that involves the central as well as the peripheral nervous system.
Copyright © 2021, Otology & Neurotology, Inc.
Conflict of interest statement
The authors disclose no conflicts of interest.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
