

The Estimated Number and Lifetime Medical Cost of HIV Infections Attributable to Sexually Transmitted Infections Acquired in the United States in 2018: A Compilation of Published Modeling Results
- PMID: 33492098
- PMCID: PMC10676007
- DOI: 10.1097/OLQ.0000000000001358
The Estimated Number and Lifetime Medical Cost of HIV Infections Attributable to Sexually Transmitted Infections Acquired in the United States in 2018: A Compilation of Published Modeling Results
Abstract
Background: The purpose of this study was to estimate the number and lifetime medical cost of HIV infections attributable to incident sexually transmitted infections (STIs) in the United States in 2018.
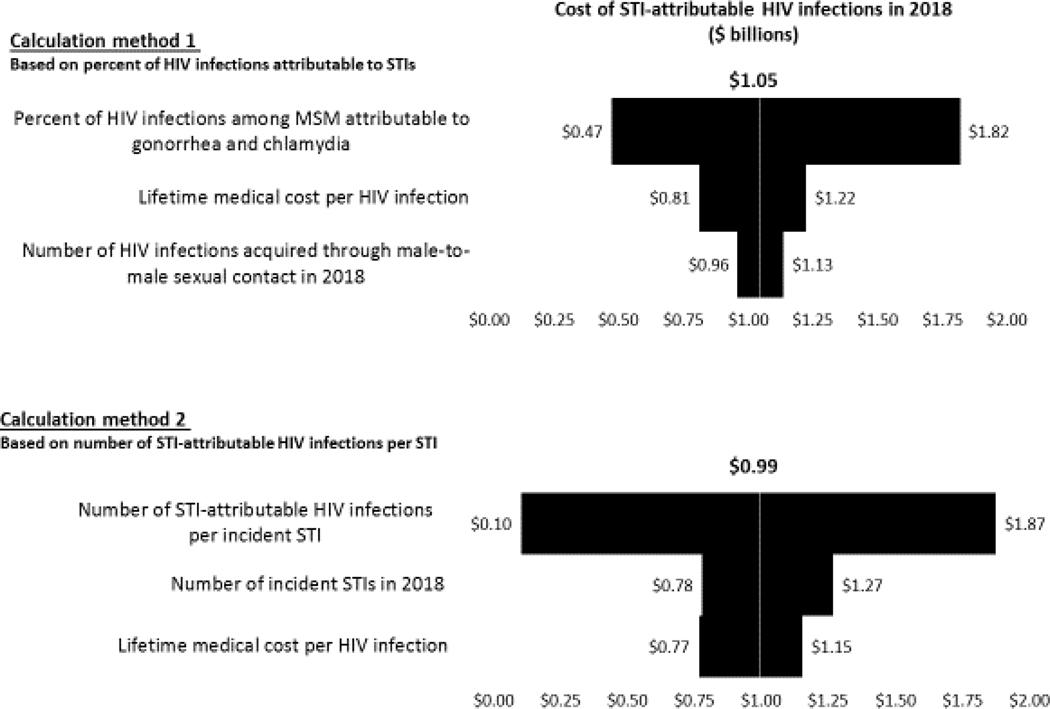
Methods: We combined data from published models regarding the number or percentage of HIV infections attributable to STIs with updated estimates of the lifetime medical cost per HIV infection. We used 2 distinct calculation methods. Our first calculation used recent estimates of the percentage of HIV infections in men who have sex with men (MSM) attributable to gonorrhea and chlamydia. Our second calculation, based on older studies, used estimates of the expected number of STI-attributable HIV infections per new STI infection, for gonorrhea, chlamydia, syphilis, and trichomoniasis.
Results: Our first calculation method suggested that 2489 (25th-75th percentiles, 1895-3000) HIV infections in 2018 among MSM could be attributed to gonorrhea and chlamydia, at an estimated lifetime medical cost of $1.05 billion (25th-75th percentiles, $0.79-$1.26 billion). Our second calculation method suggested that 2349 (25th-75th percentiles, 1948-2744) HIV infections in the general population (including MSM) could be attributed to chlamydia, gonorrhea, syphilis, and trichomoniasis acquired in 2018, at an estimated lifetime medical cost of $0.99 billion (25th-75th percentiles, $0.80-$1.16 billion).
Conclusions: Despite ambiguity regarding the degree to which STIs affect HIV transmission, our combination of data from published STI/HIV transmission models and an HIV lifetime medical cost model can help to quantify the estimated burden of STI-attributable HIV infections in the United States.
Copyright © 2021 American Sexually Transmitted Diseases Association. All rights reserved.
Conflict of interest statement
Conflict of Interest and Sources of Funding: None declared.
Figures
Similar articles
-
The Estimated Direct Lifetime Medical Costs of Sexually Transmitted Infections Acquired in the United States in 2018.Sex Transm Dis. 2021 Apr 1;48(4):215-221. doi: 10.1097/OLQ.0000000000001380. Sex Transm Dis. 2021. PMID: 33492093 Free PMC article.
-
Understanding dynamics and overlapping epidemiologies of HIV, HSV-2, chlamydia, gonorrhea, and syphilis in sexual networks of men who have sex with men.Front Public Health. 2024 Apr 2;12:1335693. doi: 10.3389/fpubh.2024.1335693. eCollection 2024. Front Public Health. 2024. PMID: 38628844 Free PMC article.
-
Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2018.Sex Transm Dis. 2021 Apr 1;48(4):208-214. doi: 10.1097/OLQ.0000000000001355. Sex Transm Dis. 2021. PMID: 33492089 Free PMC article.
-
Diagnosis and Treatment of Sexually Transmitted Infections: A Review.JAMA. 2022 Jan 11;327(2):161-172. doi: 10.1001/jama.2021.23487. JAMA. 2022. PMID: 35015033 Review.
-
Sexually transmitted infections among US women and men: prevalence and incidence estimates, 2008.Sex Transm Dis. 2013 Mar;40(3):187-93. doi: 10.1097/OLQ.0b013e318286bb53. Sex Transm Dis. 2013. PMID: 23403598 Review.
Cited by
-
An Updated Spreadsheet Tool to Estimate the Health and Economic Benefits of Sexually Transmitted Infection and HIV Prevention Activities.Sex Transm Dis. 2025 Aug 1;52(8):443-449. doi: 10.1097/OLQ.0000000000002147. Epub 2025 Mar 3. Sex Transm Dis. 2025. PMID: 40028923 Free PMC article.
-
An Interactive Modeling Tool for Projecting the Health and Direct Medical Cost Impact of Changes in the Sexually Transmitted Diseases Prevention Program Budgets.J Public Health Manag Pract. 2024 Mar-Apr 01;30(2):221-230. doi: 10.1097/PHH.0000000000001868. J Public Health Manag Pract. 2024. PMID: 38271104 Free PMC article.
-
The Estimated Direct Lifetime Medical Costs of Sexually Transmitted Infections Acquired in the United States in 2018.Sex Transm Dis. 2021 Apr 1;48(4):215-221. doi: 10.1097/OLQ.0000000000001380. Sex Transm Dis. 2021. PMID: 33492093 Free PMC article.
-
Estimated costs and quality-adjusted life-years lost due to N. gonorrhoeae infections acquired in 2015 in the United States: A modelling study of overall burden and disparities by age, race/ethnicity, and other factors.Lancet Reg Health Am. 2022 Sep 5;16:100364. doi: 10.1016/j.lana.2022.100364. eCollection 2022 Dec. Lancet Reg Health Am. 2022. PMID: 36777156 Free PMC article.
References
-
- Bernstein KT, Marcus JL, Nieri G, et al. Rectal gonorrhea and chlamydia reinfection is associated with increased risk of HIV seroconversion. JAIDS 2010;53:537–543. - PubMed
-
- Røttingen JA, Cameron DW, Garnett GP. A systematic review of the epidemiologic interactions between classic sexually transmitted diseases and HIV: how much really is known? Sex Transm Dis 2001;28:579–597. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
