

Population vs Individual Prediction of Poor Health From Results of Adverse Childhood Experiences Screening
- PMID: 33492366
- PMCID: PMC7835926
- DOI: 10.1001/jamapediatrics.2020.5602
Population vs Individual Prediction of Poor Health From Results of Adverse Childhood Experiences Screening
Abstract
Importance: Adverse childhood experiences (ACEs) are well-established risk factors for health problems in a population. However, it is not known whether screening for ACEs can accurately identify individuals who develop later health problems.
Objective: To test the predictive accuracy of ACE screening for later health problems.
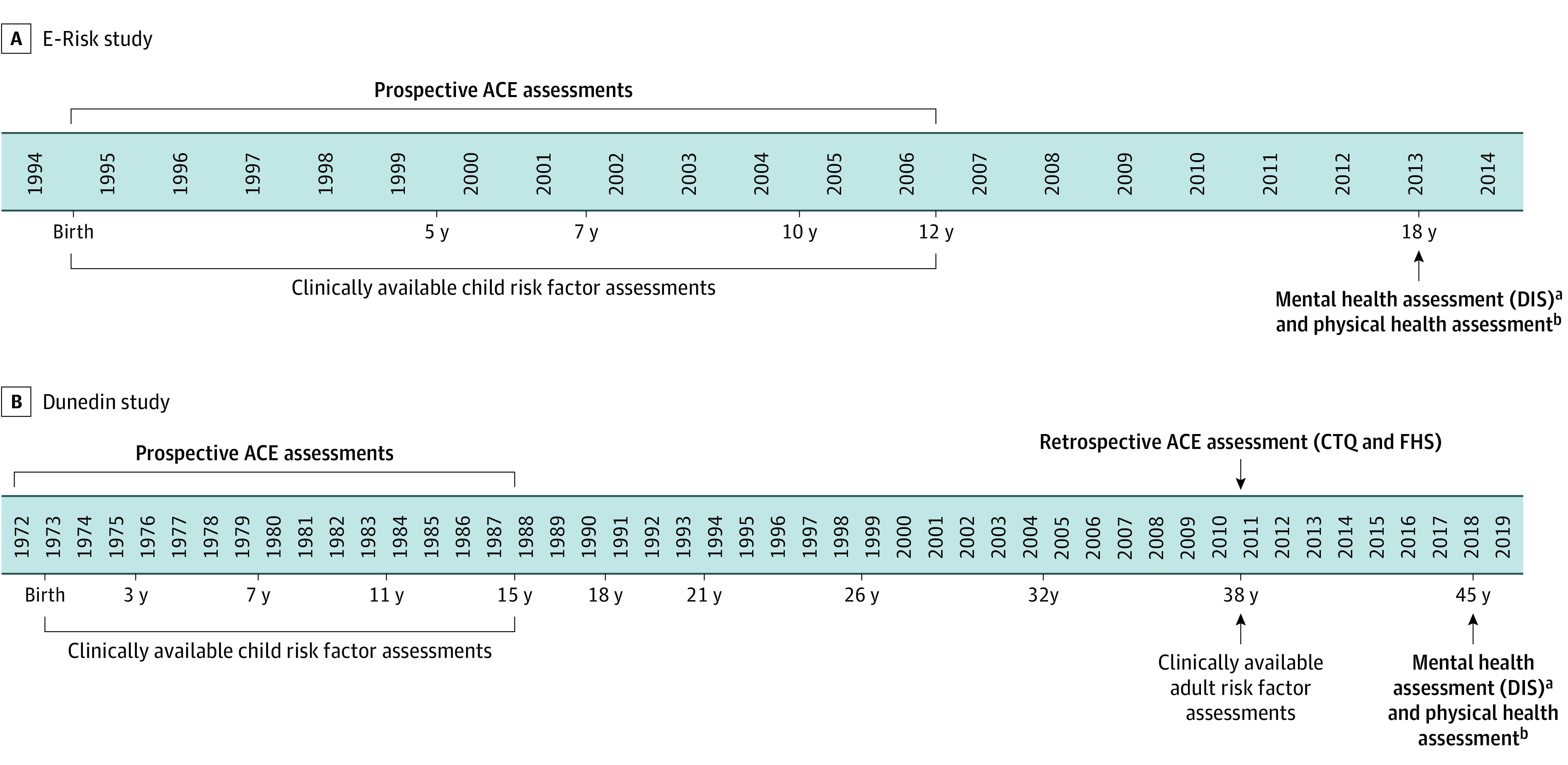
Design, setting, and participants: This study comprised 2 birth cohorts: the Environmental Risk (E-Risk) Longitudinal Twin Study observed 2232 participants born during the period from 1994 to 1995 until they were aged 18 years (2012-2014); the Dunedin Multidisciplinary Health and Development Study observed 1037 participants born during the period from 1972 to 1973 until they were aged 45 years (2017-2019). Statistical analysis was performed from May 28, 2018, to July 29, 2020.
Exposures: ACEs were measured prospectively in childhood through repeated interviews and observations in both cohorts. ACEs were also measured retrospectively in the Dunedin cohort through interviews at 38 years.
Main outcomes and measures: Health outcomes were assessed at 18 years in E-Risk and at 45 years in the Dunedin cohort. Mental health problems were assessed through clinical interviews using the Diagnostic Interview Schedule. Physical health problems were assessed through interviews, anthropometric measurements, and blood collection.
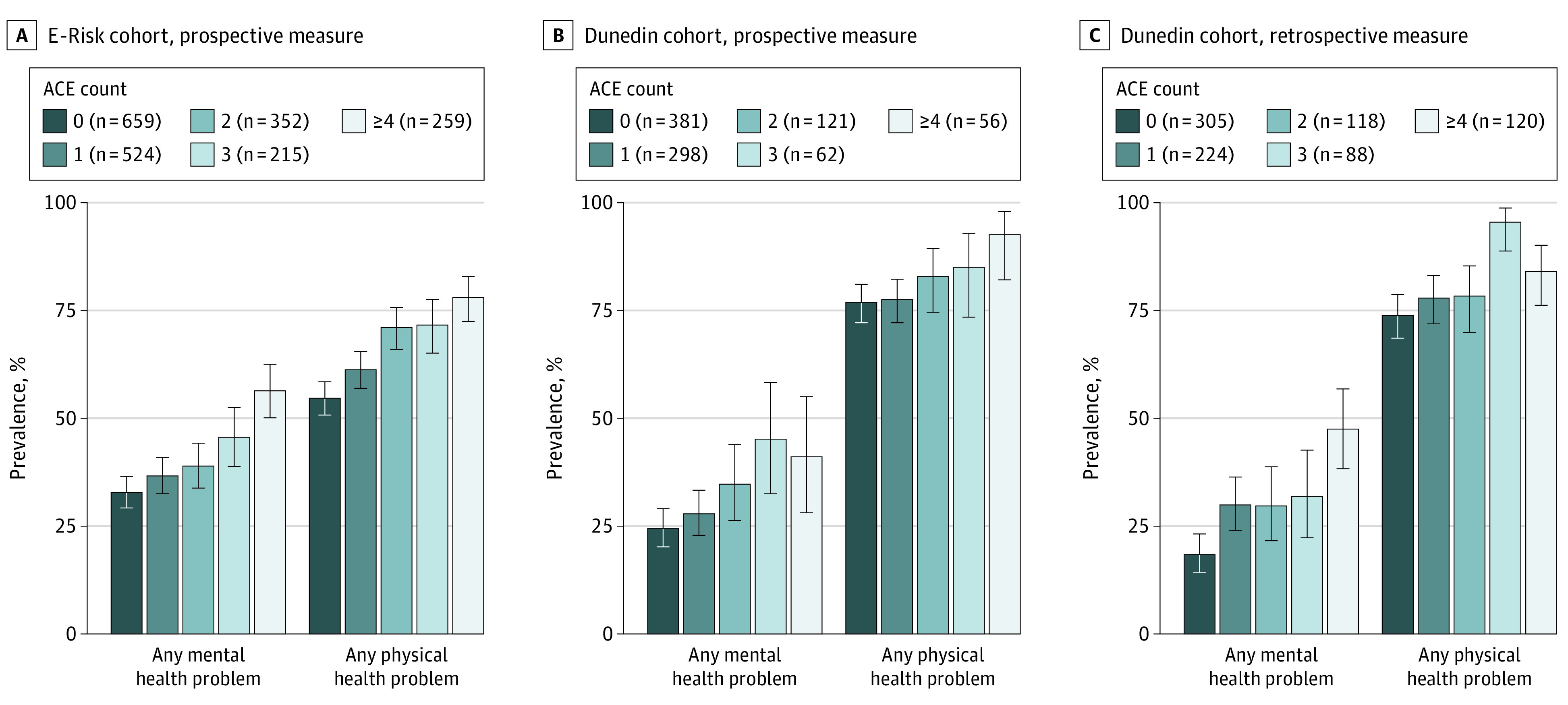
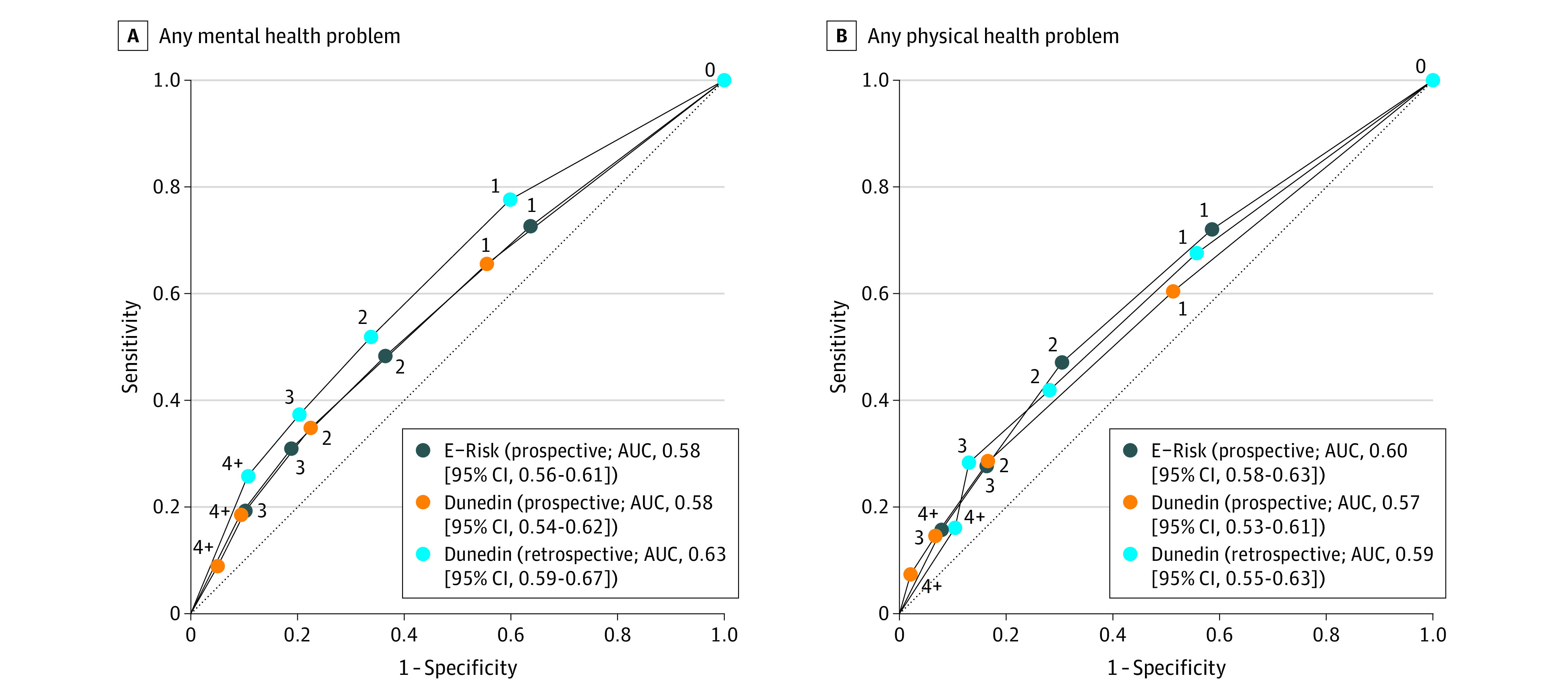
Results: Of 2232 E-Risk participants, 2009 (1051 girls [52%]) were included in the analysis. Of 1037 Dunedin cohort participants, 918 (460 boys [50%]) were included in the analysis. In E-Risk, children with higher ACE scores had greater risk of later health problems (any mental health problem: relative risk, 1.14 [95% CI, 1.10-1.18] per each additional ACE; any physical health problem: relative risk, 1.09 [95% CI, 1.07-1.12] per each additional ACE). ACE scores were associated with health problems independent of other information typically available to clinicians (ie, sex, socioeconomic disadvantage, and history of health problems). However, ACE scores had poor accuracy in predicting an individual's risk of later health problems (any mental health problem: area under the receiver operating characteristic curve, 0.58 [95% CI, 0.56-0.61]; any physical health problem: area under the receiver operating characteristic curve, 0.60 [95% CI, 0.58-0.63]; chance prediction: area under the receiver operating characteristic curve, 0.50). Findings were consistent in the Dunedin cohort using both prospective and retrospective ACE measures.
Conclusions and relevance: This study suggests that, although ACE scores can forecast mean group differences in health, they have poor accuracy in predicting an individual's risk of later health problems. Therefore, targeting interventions based on ACE screening is likely to be ineffective in preventing poor health outcomes.
Conflict of interest statement
Figures
Comment in
-
Research, Practice, and Policy Implications of Adverse Childhood Events.JAMA Pediatr. 2021 Aug 1;175(8):866-867. doi: 10.1001/jamapediatrics.2021.0810. JAMA Pediatr. 2021. PMID: 33970184 No abstract available.
-
Research, Practice, and Policy Implications of Adverse Childhood Events-Reply.JAMA Pediatr. 2021 Aug 1;175(8):867-868. doi: 10.1001/jamapediatrics.2021.0813. JAMA Pediatr. 2021. PMID: 33970203 No abstract available.
References
-
- Bellis MA, Hughes K, Ford K, Ramos Rodriguez G, Sethi D, Passmore J. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. Lancet Public Health. 2019;4(10):e517-e528. doi: 10.1016/S2468-2667(19)30145-8 - DOI - PMC - PubMed
-
- Garner AS, Shonkoff JP, Siegel BS, et al. ; Committee on Psychosocial Aspects of Child and Family Health; Committee on Early Childhood, Adoption, and Dependent Care; Section on Developmental and Behavioral Pediatrics . Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics. 2012;129(1):e224-e231. doi: 10.1542/peds.2011-2662 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
