

Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models: positioning the middle colic artery bifurcation and its relevance to surgeons operating colon cancer
- PMID: 33492511
- PMCID: PMC8741724
- DOI: 10.1007/s00464-020-08242-8
Re-interpreting mesenteric vascular anatomy on 3D virtual and/or physical models: positioning the middle colic artery bifurcation and its relevance to surgeons operating colon cancer
Abstract
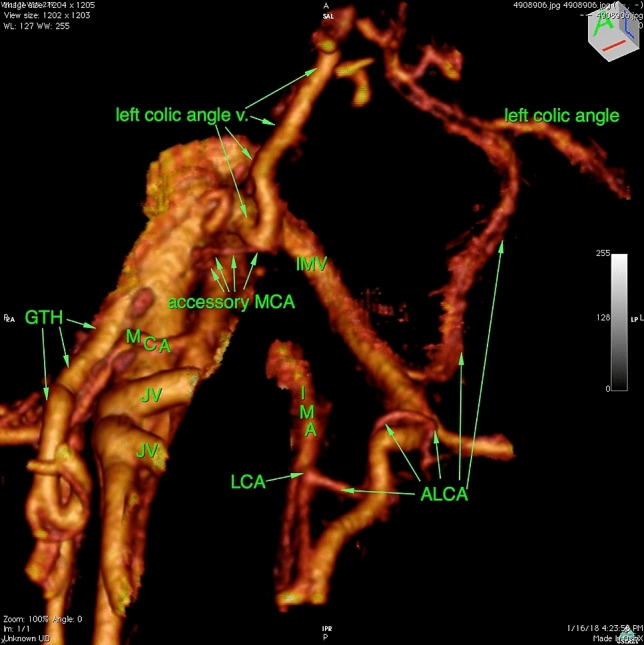
Background: The impact of the position of the middle colic artery (MCA) bifurcation and the trajectory of the accessory MCA (aMCA) on adequate lymphadenectomy when operating colon cancer have as of yet not been described and/or analysed in the literature. The aim of this study was to determine the MCA bifurcation position to anatomical landmarks and to assess the trajectory of aMCA.
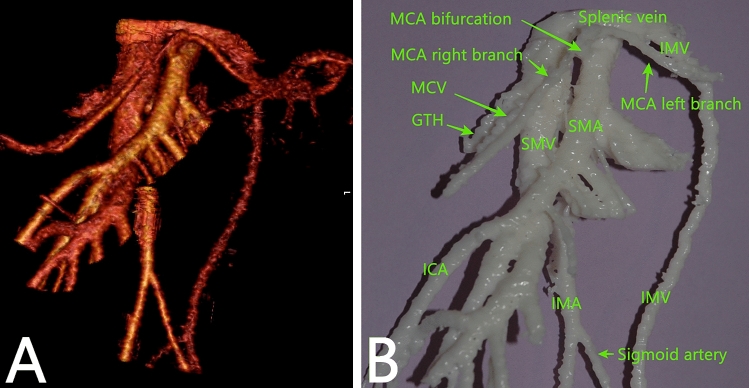
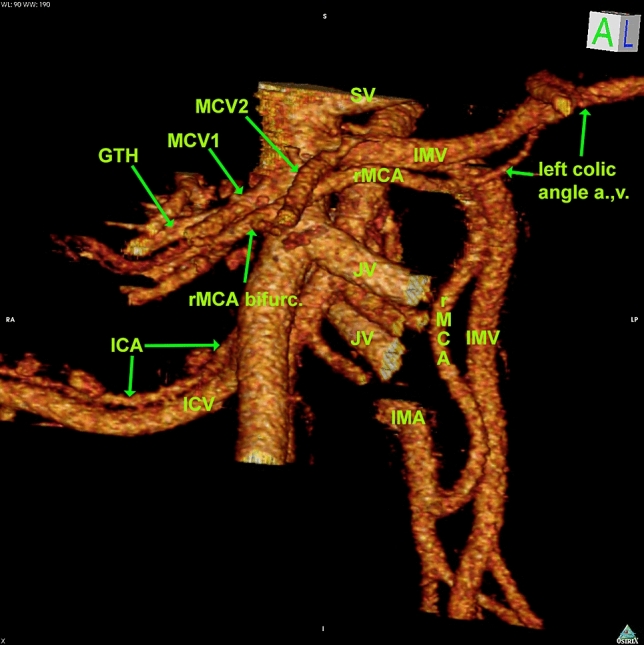
Methods: The colonic vascular anatomy was manually reconstructed in 3D from high-resolution CT datasets using Osirix MD and 3-matic Medical and analysed. CT datasets were exported as STL files and supplemented with 3D printed models when required.
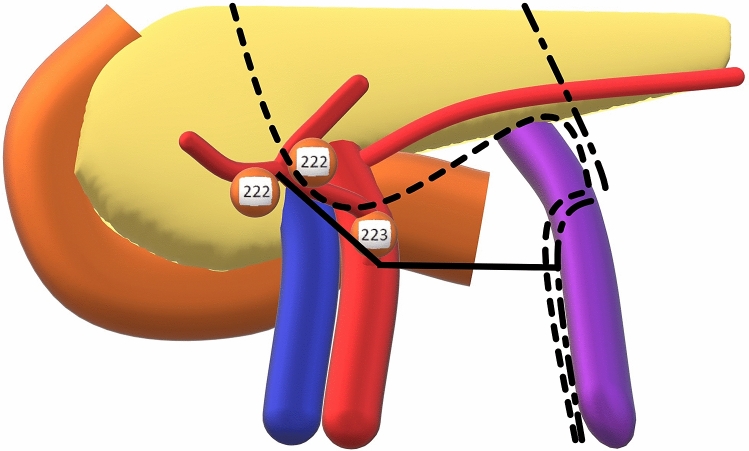
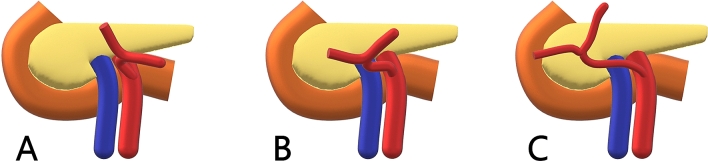
Results: Thirty-two datasets were analysed. The MCA bifurcation was left to the superior mesenteric vein (SMV) in 4 (12.1%), in front of SMV in 17 (53.1%) and right to SMV in 11 (34.4%) models. Median distances from the MCA origin to bifurcation were 3.21 (1.18-15.60) cm. A longer MCA bifurcated over or right to SMV, while a shorter bifurcated left to SMV (r = 0.457, p = 0.009). The main MCA direction was towards right in 19 (59.4%) models. When initial directions included left, the bifurcation occurred left to or anterior to SMV in all models. When the initial directions included right, the bifurcation occurred anterior or right to SMV in all models. The aMCA was found in 10 (31.3%) models, following the inferior mesenteric vein (IMV) in 5 near the lower pancreatic border. The IMV confluence was into SMV in 18 (56.3%), splenic vein in 11 (34.4%) and jejunal vein in 3 (9.4%) models.
Conclusion: Awareness of the wide range of MCA bifurcation positions reported is crucial for the quality of lymphadenectomy performed. The aMCA occurs in 31.3% models and its trajectory is in proximity to the lower pancreatic border in one half of models, indicating that it needs to be considered when operating splenic flexure cancer.
Keywords: 3D printing; Accessory middle colic artery; Colonic cancer surgery; Left colectomy; Mesenteric vascular anatomy; Middle colic artery; Splenic flexure cancer.
© 2021. The Author(s).
Conflict of interest statement
Bjarte T. Andersen, Bojan V. Stimec, Bjørn Edwin, Airazat M. Kazaryan, Przemyslaw J. Maziarz and Dejan Ignjatovic report any conflict of interest or financial disclosures.
Figures
References
-
- Hohenberger W, Weber K, Matzel K, Papadopoulos T, Merkel S. Standardized surgery for colonic cancer: complete mesocolic excision and central ligation–technical notes and outcome. Colorectal Dis. 2009;11(4):354–364. - PubMed
-
- Coffey JC, Sehgal R, Culligan K, Dunne C, McGrath D, Lawes N, Walsh D. Terminology and nomenclature in colonic surgery: universal application of a rule-based approach derived from updates on mesenteric anatomy. Tech Coloproctol. 2014;18(9):789–794. - PubMed
-
- West NP, Hohenberger W, Weber K, Perrakis A, Finan PJ, Quirke P. Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol. 2010;28(2):272–278. - PubMed
-
- Nesgaard JM, Stimec BV, Bakka AO, Edwin B, Ignjatovic D. Navigating the mesentery: a comparative pre- and per-operative visualization of the vascular anatomy. Colorectal Dis. 2015;17(9):810–819. - PubMed
-
- Nesgaard JM, Stimec BV, Ignjatovic D. Is tracing vessels to the origin in right colectomy really impossible? Dis Colon Rectum. 2017;60(8):e607–e608. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
