

Intrapartum Antibiotic Exposure and Body Mass Index in Children
- PMID: 33493270
- PMCID: PMC11309029
- DOI: 10.1093/cid/ciab053
Intrapartum Antibiotic Exposure and Body Mass Index in Children
Abstract
Background: Intrapartum antibiotic prophylaxis (IAP) reduces a newborn's risk of group B streptococcal infection (GBS) but may lead to an increased childhood body mass index (BMI).
Methods: This was a retrospective cohort study of infants (n = 223 431) born 2007-2015 in an integrated healthcare system. For vaginal delivery, we compared children exposed to GBS-IAP and to any other type or duration of intrapartum antibiotics to no antibiotic exposure. For cesarean delivery, we compared children exposed to GBS-IAP to those exposed to all other intrapartum antibiotics, including surgical prophylaxis. BMI over 5 years was compared using nonlinear multivariate models with B-spline functions, stratified by delivery mode and adjusted for demographics, maternal factors, breastfeeding, and childhood antibiotic exposure.
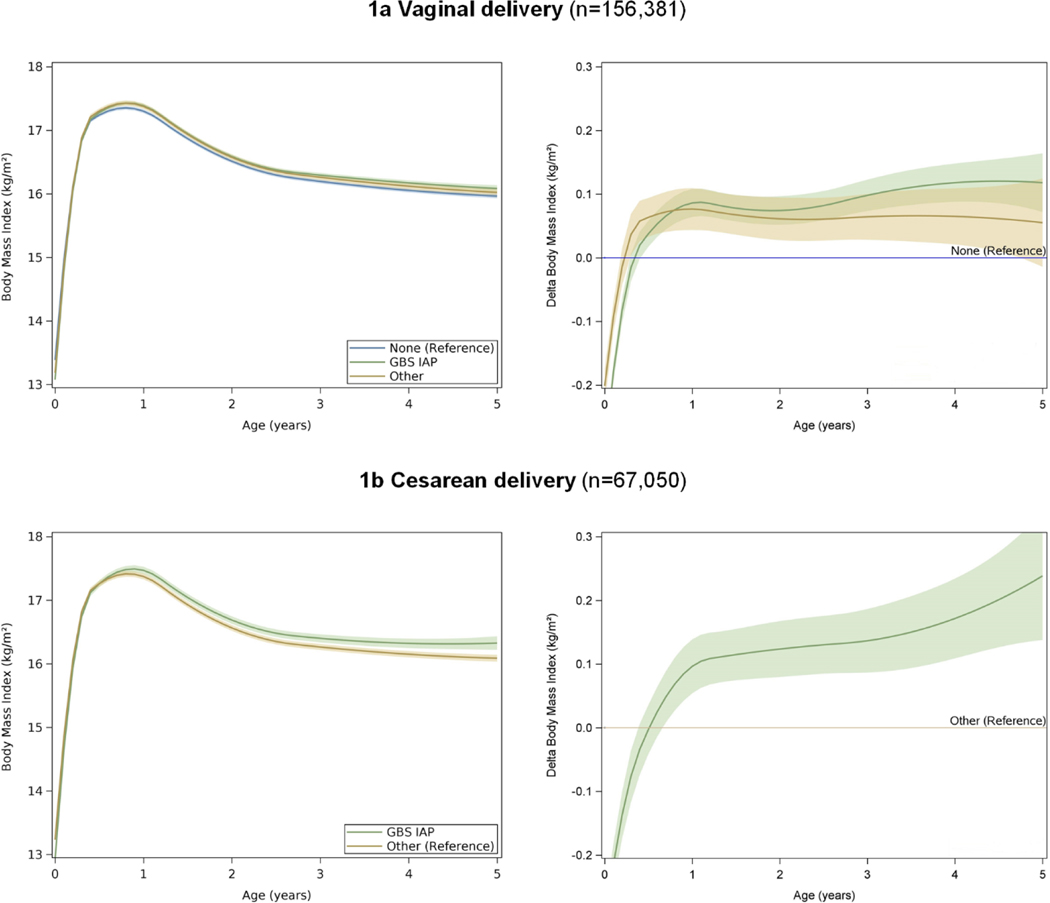
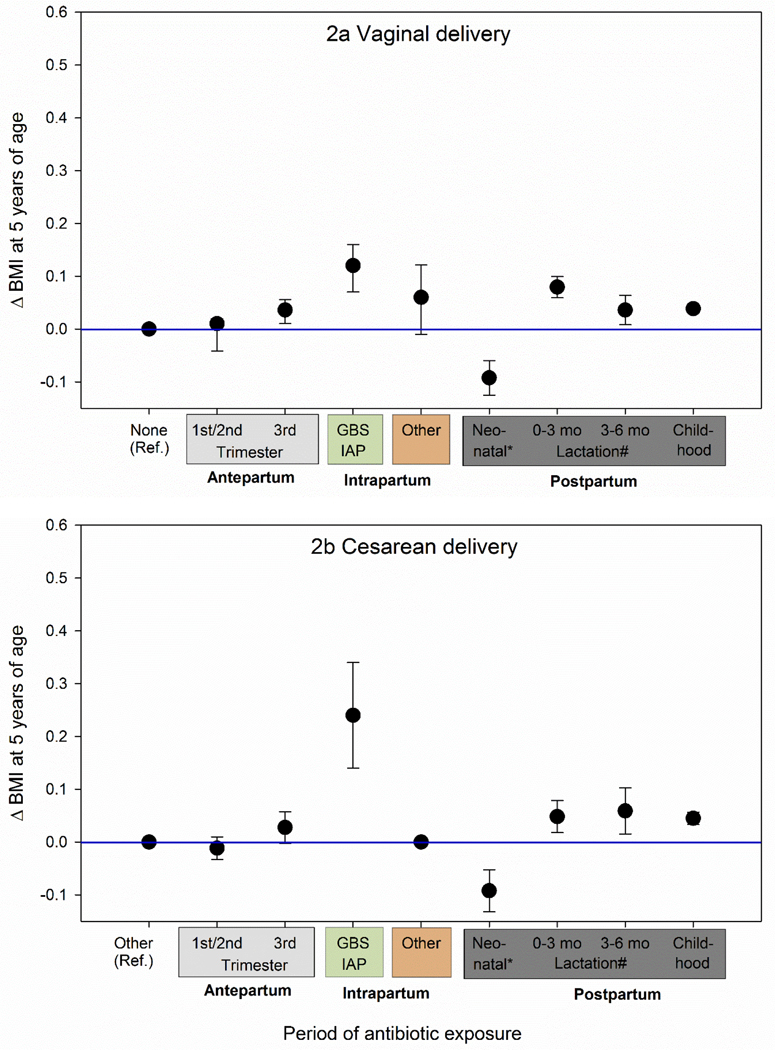
Results: In vaginal deliveries, GBS-IAP was associated with higher BMI from 0.5 to 5.0 years of age compared to no antibiotics (P < .0001 for all time points, ΔBMI at age 5 years 0.12 kg/m2, 95% confidence interval [CI]: .07-.16 kg/m2). Other antibiotics were associated with higher BMI from 0.3 to 5.0 years of age. In cesarean deliveries, GBS-IAP was associated with increased BMI from 0.7 years to 5.0 years of age (P < .05 for 0.7-0.8 years, P < .0001 for all other time points) compared to other antibiotics (ΔBMI at age 5 years 0.24 kg/m2, 95% CI: .14-.34 kg/m2). Breastfeeding did not modify these associations.
Conclusions: GBS-IAP was associated with a small but sustained increase in BMI starting at very early age. This association highlights the need to better understand the effects of perinatal antibiotic exposure on childhood health.
Keywords: body mass index; childhood obesity; delivery mode; intrapartum antibiotic prophylaxis.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
