

The Epidemiology of UK Autoimmune Liver Disease Varies With Geographic Latitude
- PMID: 33493696
- PMCID: PMC8661127
- DOI: 10.1016/j.cgh.2021.01.029
The Epidemiology of UK Autoimmune Liver Disease Varies With Geographic Latitude
Abstract
Background & aims: The epidemiology of autoimmune liver disease (AILD) is challenging to study because of the diseases' rarity and because of cohort selection bias. Increased incidence farther from the Equator has been reported for multiple sclerosis, another autoimmune disease. We assessed the incidence of primary biliary cholangitis (PBC), primary sclerosing cholangitis (PSC), and autoimmune hepatitis (AIH) in relation to latitude.
Methods: We performed a retrospective cohort study using anonymized UK primary care records from January 1, 2002, to May 10, 2016. All adults without a baseline diagnosis of AILD were included and followed up until the first occurrence of an AILD diagnosis, death, or they left the database. Latitude was measured as registered general practice rounded down to whole degrees.
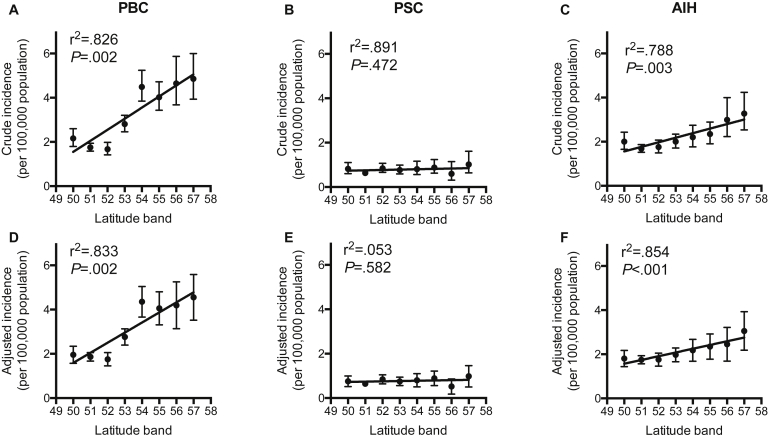
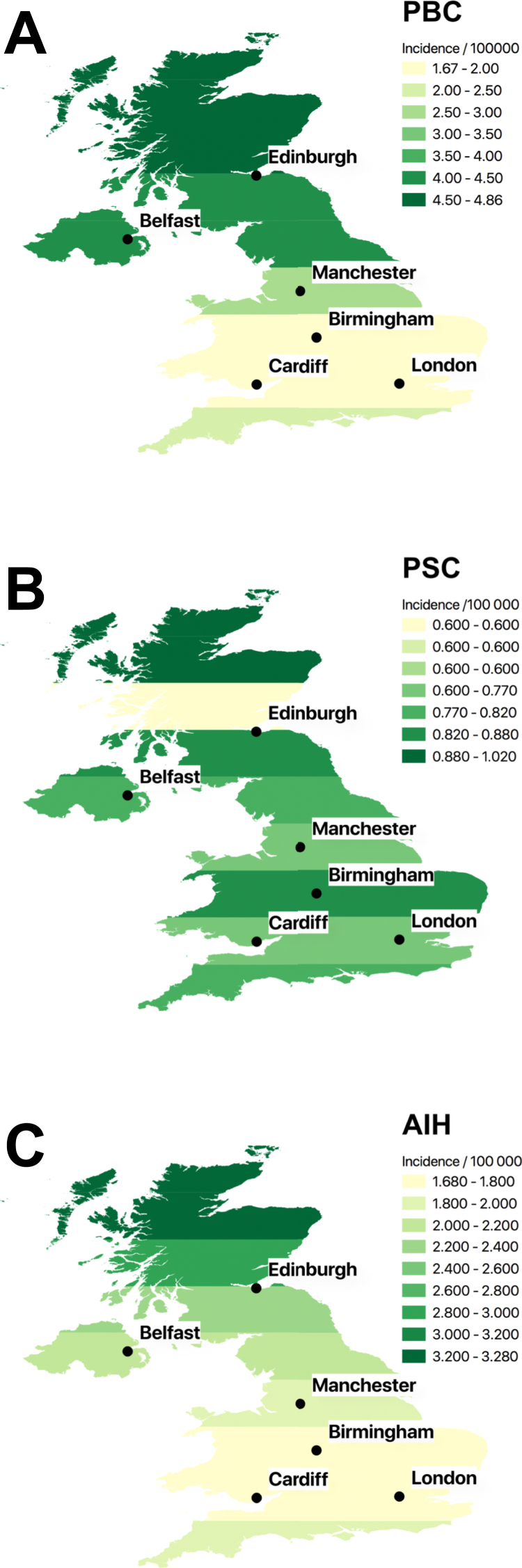
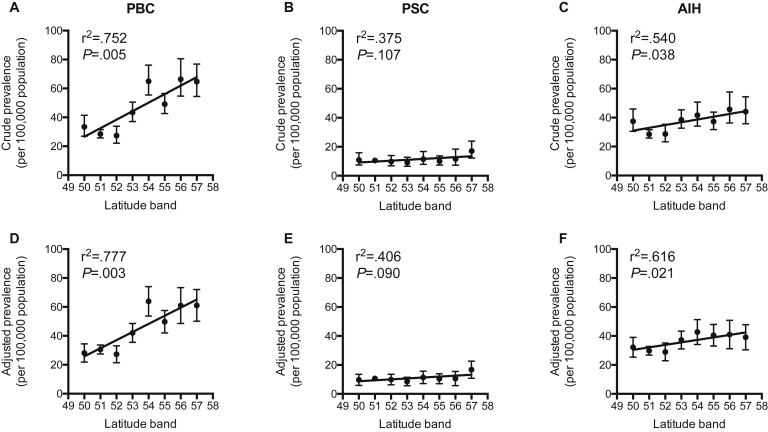
Results: The cohort included 8,590,421 records with 53.3 × 107 years of follow-up evaluation from 694 practices. There were 1314 incident cases of PBC, 396 of PSC, and 1034 of AIH. Crude incidences were as follows: PBC, 2.47 (95% CI, 2.34-2.60); PSC, 0.74 (95% CI, 0.67-0.82); and AIH, 1.94 (95% CI, 1.83-2.06) per 100,000 per year. PBC incidence correlated with female sex, smoking, and deprivation; PSC incidence correlated with male sex and non-smoking; AIH incidence correlated with female sex and deprivation. A more northerly latitude was associated strongly with incidence of PBC: 2.16 (95% CI, 1.79-2.60) to 4.86 (95% CI, 3.93-6.00) from 50°N to 57°N (P = .002) and incidence of AIH: 2.00 (95% CI, 1.65-2.43) to 3.28 (95% CI, 2.53-4.24) (P = .003), but not incidence of PSC: 0.82 (95% CI, 0.60-1.11) to 1.02 (95% CI, 0.64-1.61) (P = .473). Incidence after adjustment for age, sex, smoking, and deprivation status showed similar positive correlations for PBC and AIH with latitude, but not PSC. Incident AIH cases were younger at more northerly latitude.
Conclusions: We describe an association in the United Kingdom between more northerly latitude and the incidence of PBC and AIH that requires both confirmation and explanation.
Keywords: Autoimmune Hepatitis; Autoimmune Liver Disease; Latitude; Primary Biliary Cholangitis; Primary Sclerosing Cholangitis.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Hirschfield G.M., Karlsen T.H., Lindor K.D., et al. Primary sclerosing cholangitis. Lancet. 2013;382:1587–1599. - PubMed
-
- Hirschfield G.M., Gershwin M.E. The immunobiology and pathophysiology of primary biliary cirrhosis. Annu Rev Pathol. 2013;8:303–330. - PubMed
-
- Webb G.J., Hirschfield G.M., Krawitt E.L., et al. Cellular and molecular mechanisms of autoimmune hepatitis. Annu Rev Pathol. 2018;13:247–292. - PubMed
-
- Webb G.J., Rana A., Hodson J., et al. Twenty-year comparative analysis of patients with autoimmune liver diseases on transplant waitlists. Clin Gastroenterol Hepatol. 2018;16:278–287 e7. - PubMed
-
- Boonstra K., Beuers U., Ponsioen C.Y. Epidemiology of primary sclerosing cholangitis and primary biliary cirrhosis: a systematic review. J Hepatol. 2012;56:1181–1188. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
