

Global absence and targeting of protective immune states in severe COVID-19
- PMID: 33494096
- PMCID: PMC8567458
- DOI: 10.1038/s41586-021-03234-7
Global absence and targeting of protective immune states in severe COVID-19
Erratum in
-
Publisher Correction: Global absence and targeting of protective immune states in severe COVID-19.Nature. 2021 Aug;596(7872):E8. doi: 10.1038/s41586-021-03718-6. Nature. 2021. PMID: 34341540 Free PMC article. No abstract available.
Abstract
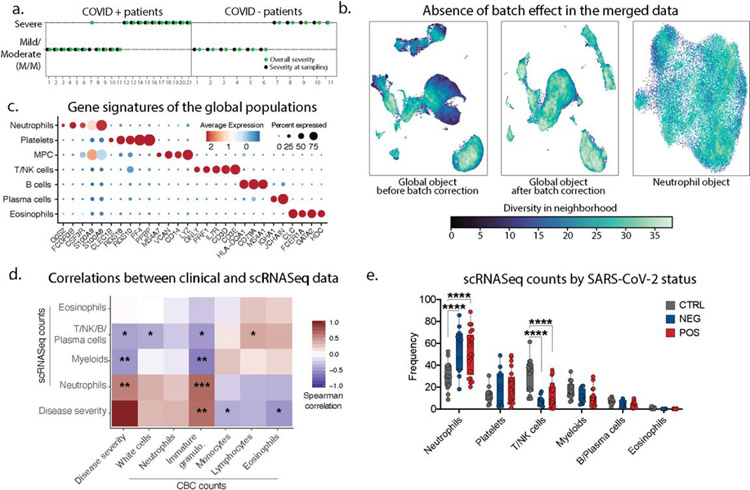
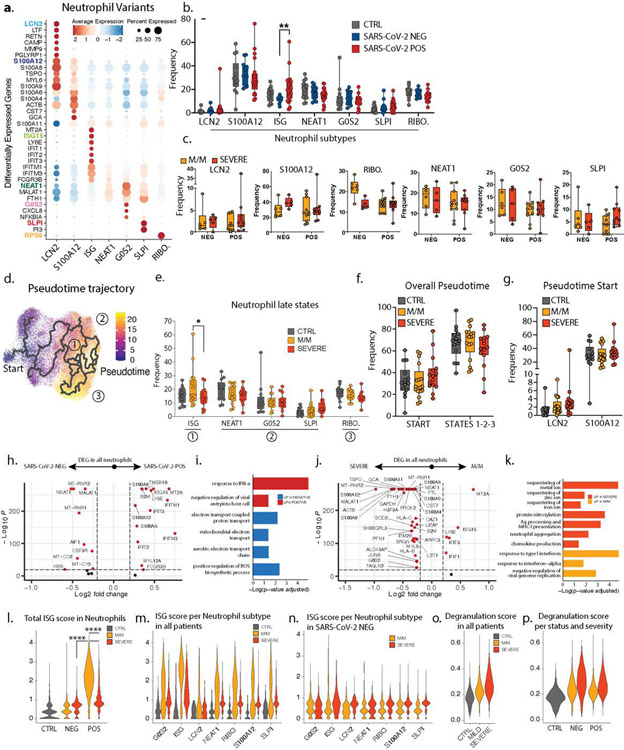
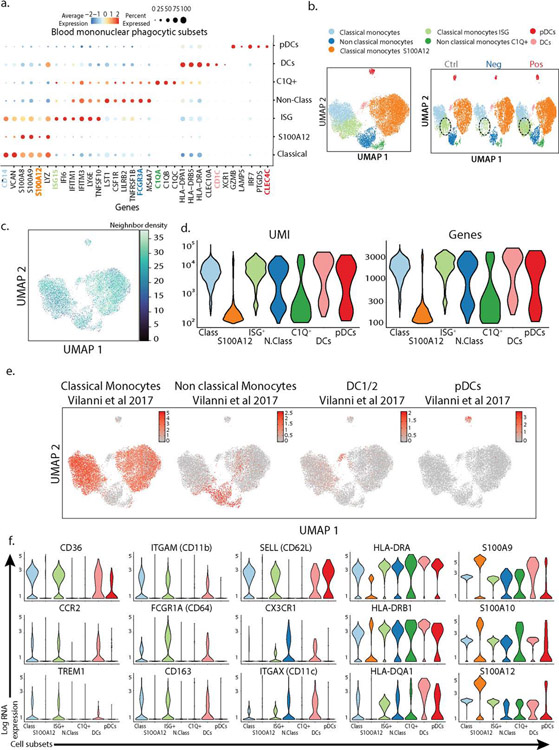
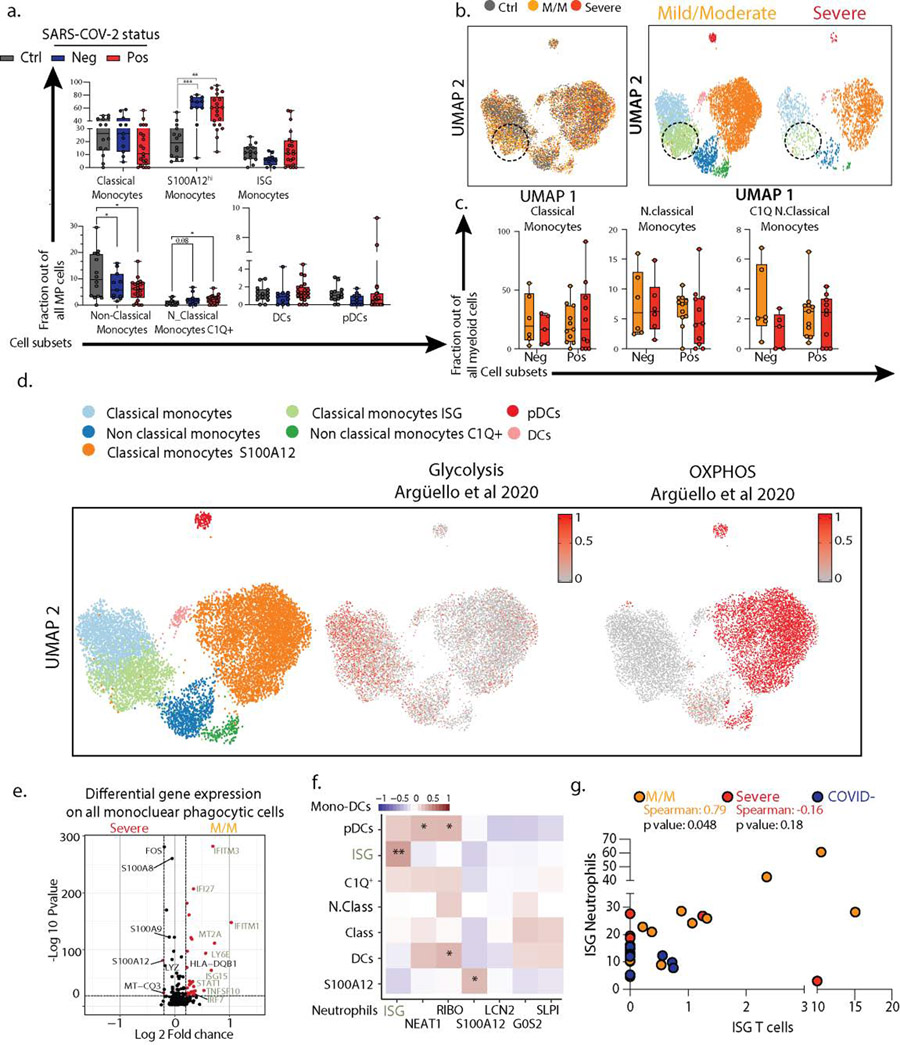
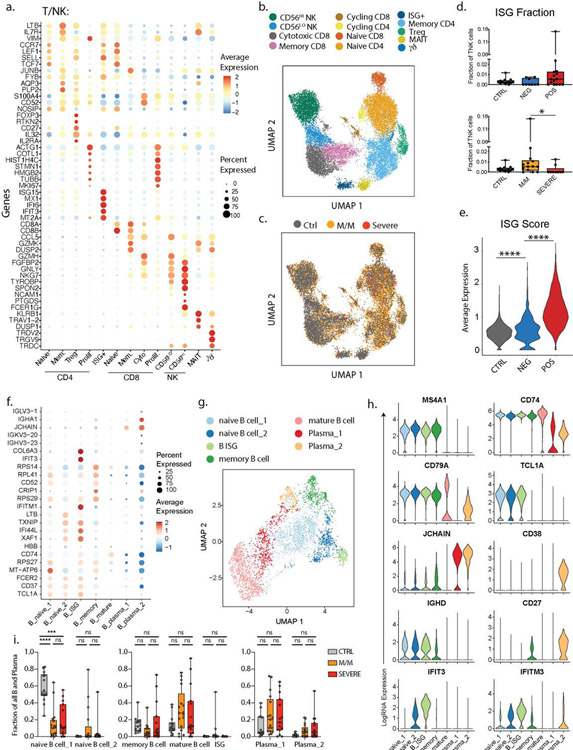
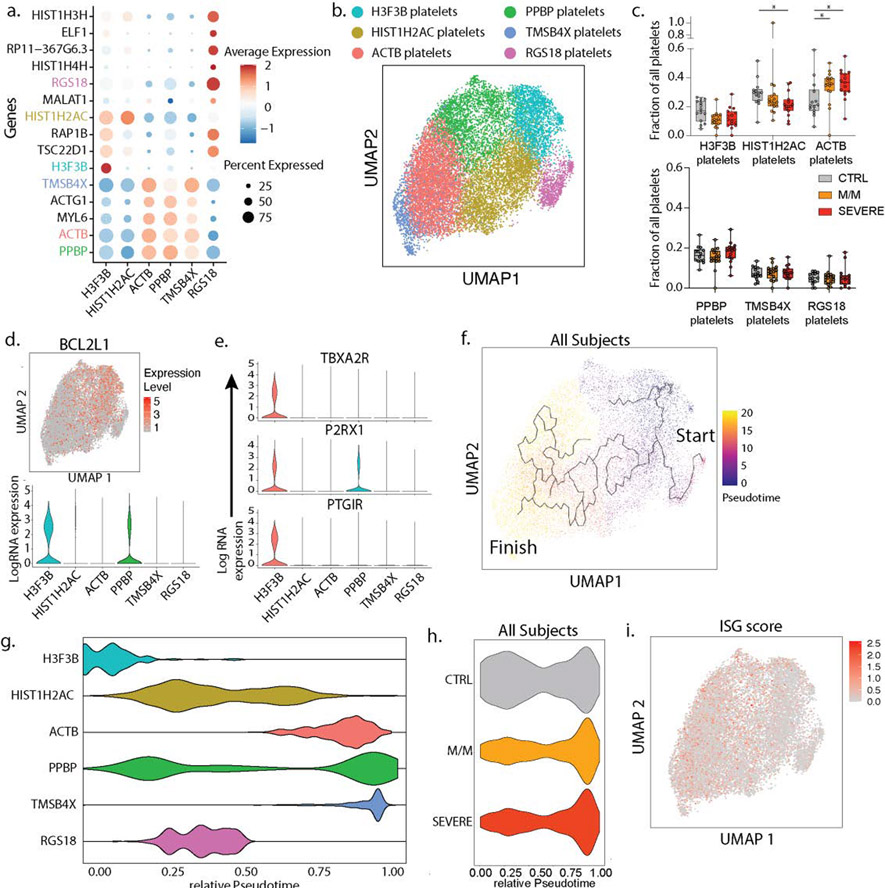
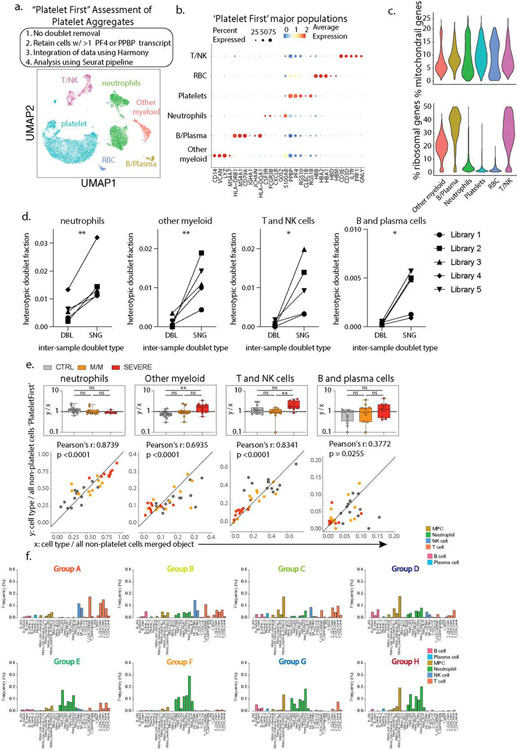
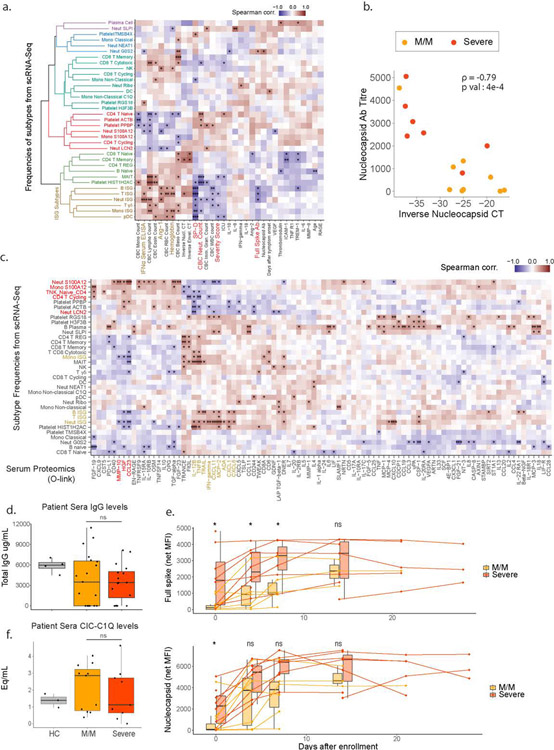
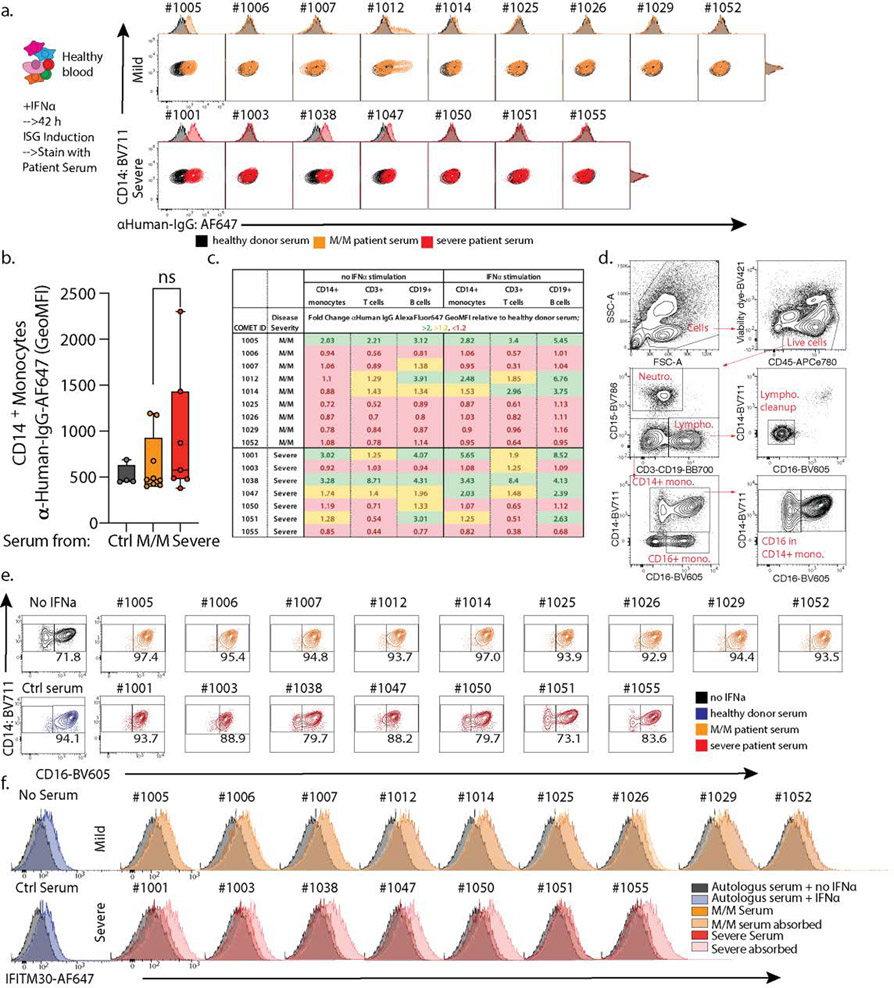
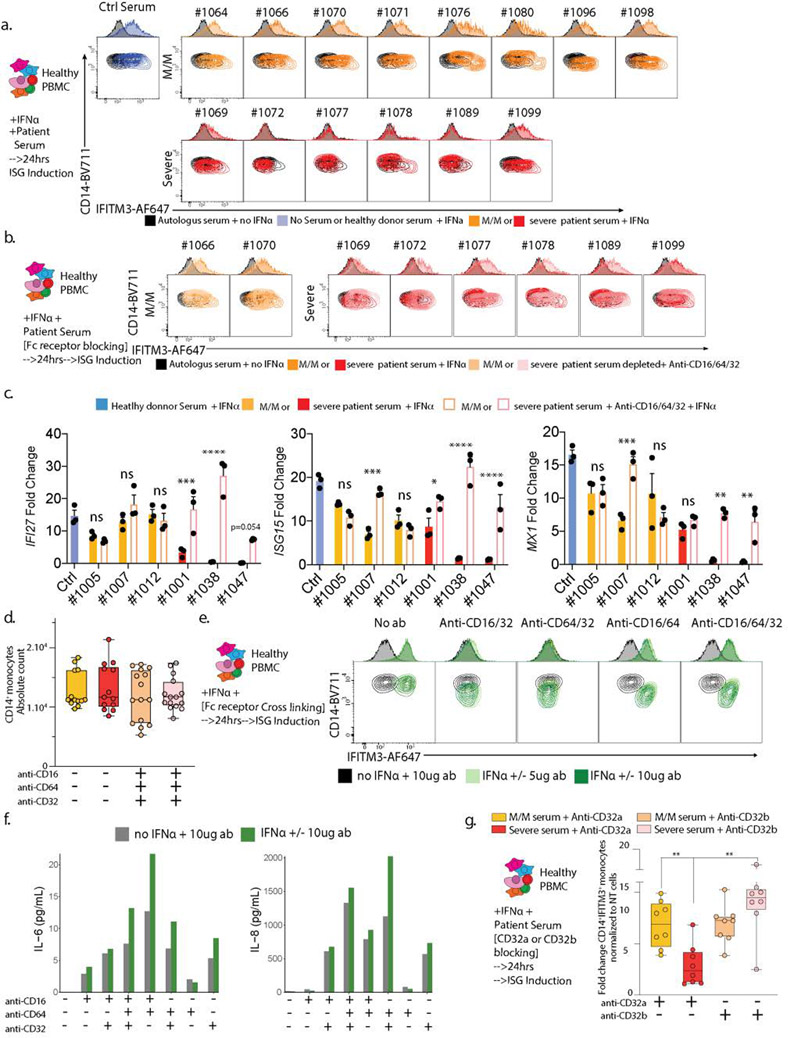
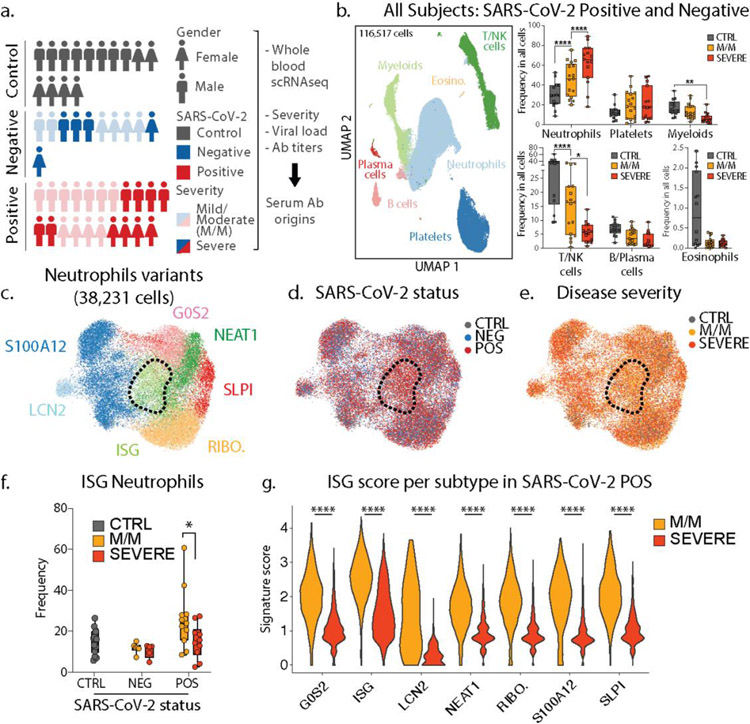
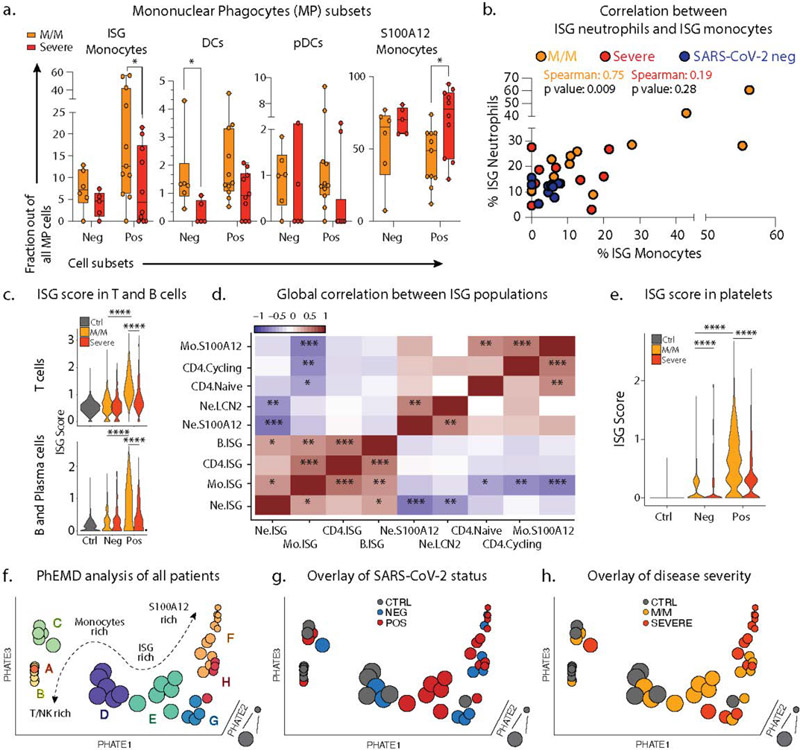
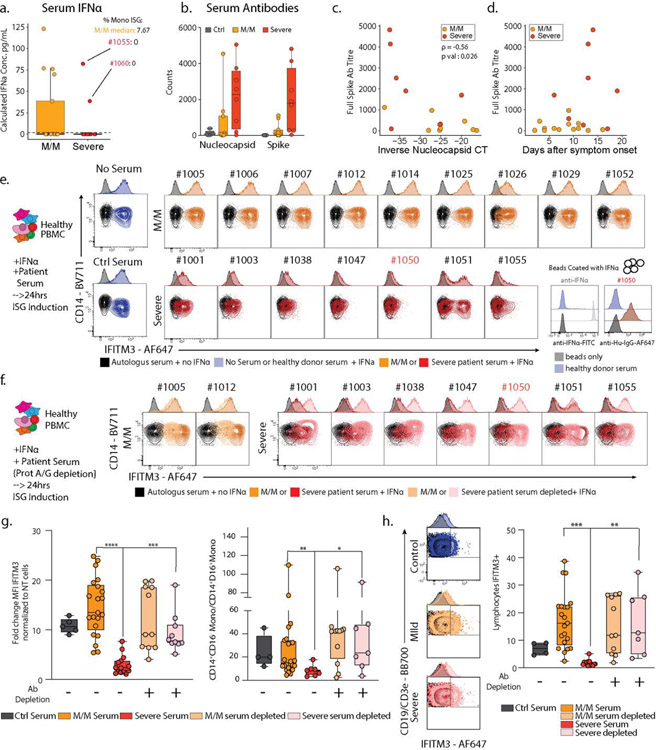
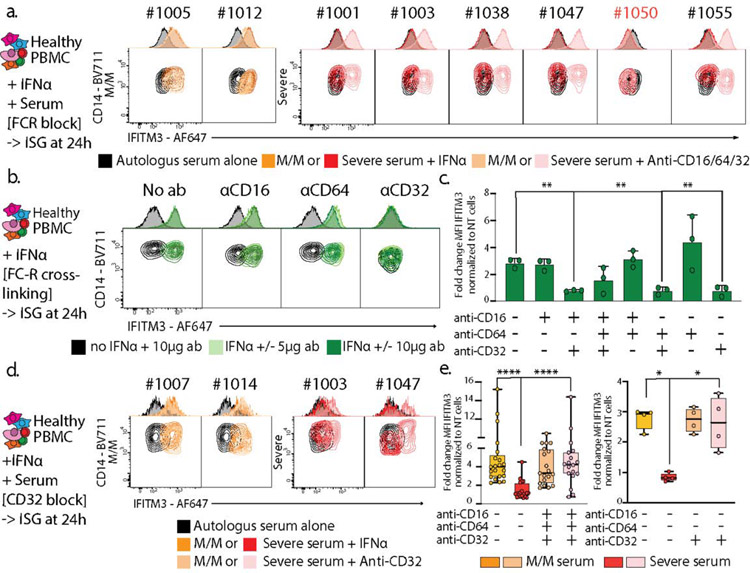
Although infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has pleiotropic and systemic effects in some individuals1-3, many others experience milder symptoms. Here, to gain a more comprehensive understanding of the distinction between severe and mild phenotypes in the pathology of coronavirus disease 2019 (COVID-19) and its origins, we performed a whole-blood-preserving single-cell analysis protocol to integrate contributions from all major immune cell types of the blood-including neutrophils, monocytes, platelets, lymphocytes and the contents of the serum. Patients with mild COVID-19 exhibit a coordinated pattern of expression of interferon-stimulated genes (ISGs)3 across every cell population, whereas these ISG-expressing cells are systemically absent in patients with severe disease. Paradoxically, individuals with severe COVID-19 produce very high titres of anti-SARS-CoV-2 antibodies and have a lower viral load compared to individuals with mild disease. Examination of the serum from patients with severe COVID-19 shows that these patients uniquely produce antibodies that functionally block the production of the ISG-expressing cells associated with mild disease, by activating conserved signalling circuits that dampen cellular responses to interferons. Overzealous antibody responses pit the immune system against itself in many patients with COVID-19, and perhaps also in individuals with other viral infections. Our findings reveal potential targets for immunotherapies in patients with severe COVID-19 to re-engage viral defence.
Conflict of interest statement
Conflict of interest Statement
The authors declare no competing financial interests.
Figures
Update of
-
Global Absence and Targeting of Protective Immune States in Severe COVID-19.Res Sq [Preprint]. 2020 Oct 28:rs.3.rs-97042. doi: 10.21203/rs.3.rs-97042/v1. Res Sq. 2020. Update in: Nature. 2021 Mar;591(7848):124-130. doi: 10.1038/s41586-021-03234-7. PMID: 33140041 Free PMC article. Updated. Preprint.
-
Global Absence and Targeting of Protective Immune States in Severe COVID-19.bioRxiv [Preprint]. 2020 Oct 29:2020.10.28.359935. doi: 10.1101/2020.10.28.359935. bioRxiv. 2020. Update in: Nature. 2021 Mar;591(7848):124-130. doi: 10.1038/s41586-021-03234-7. PMID: 33140050 Free PMC article. Updated. Preprint.
Comment in
-
Some antibodies can dampen antiviral defences in people with severe COVID.Nature. 2021 Mar;591(7848):37-39. doi: 10.1038/d41586-021-00352-0. Nature. 2021. PMID: 33654298 No abstract available.
-
FcγRIIb blockage: a promising immunotherapy target for severe COVID-19.Signal Transduct Target Ther. 2021 Apr 9;6(1):147. doi: 10.1038/s41392-021-00590-8. Signal Transduct Target Ther. 2021. PMID: 33837193 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
