

The evaluation of maximum condyle-tragus distance can predict difficult airway management without exposing upper respiratory tract; a prospective observational study
- PMID: 33494705
- PMCID: PMC7829489
- DOI: 10.1186/s12871-021-01253-5
The evaluation of maximum condyle-tragus distance can predict difficult airway management without exposing upper respiratory tract; a prospective observational study
Abstract
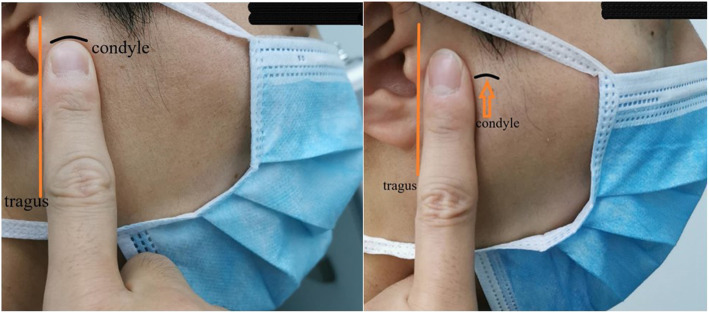
Background: Routine preoperative methods to assess airway such as the interincisor distance (IID), Mallampati classification, and upper lip bite test (ULBT) have a certain risk of upper respiratory tract exposure and virus spread. Condyle-tragus maximal distance(C-TMD) can be used to assess the airway, and does not require the patient to expose the upper respiratory tract, but its value in predicting difficult laryngoscopy compared to other indicators (Mallampati classification, IID, and ULBT) remains unknown. The purpose of this study was to observe the value of C-TMD to predict difficult laryngoscopy and the influence on intubation time and intubation attempts, and provide a new idea for preoperative airway assessment during epidemic.
Methods: Adult patients undergoing general anesthesia and tracheal intubation were enrolled. IID, Mallampati classification, ULBT, and C-TMD of each patient were evaluated before the initiation of anesthesia. The primary outcome was intubation time. The secondary outcomes were difficult laryngoscopy defined as the Cormack-Lehane Level > grade 2 and the number of intubation attempts.
Results: Three hundred four patients were successfully enrolled and completed the study, 39 patients were identified as difficult laryngoscopy. The intubation time was shorter with the C-TMD>1 finger group 46.8 ± 7.3 s, compared with the C-TMD<1 finger group 50.8 ± 8.6 s (p<0.01). First attempt success rate was higher in the C-TMD>1 finger group 98.9% than in the C-TMD<1 finger group 87.1% (P<0.01). The correlation between the C-TMD and Cormack-Lehane Level was 0.317 (Spearman correlation coefficient, P<0.001), and the area under the ROC curve was 0.699 (P<0.01). The C-TMD < 1 finger width was the most consistent with difficult laryngoscopy (κ = 0.485;95%CI:0.286-0.612) and its OR value was 10.09 (95%CI: 4.19-24.28), sensitivity was 0.469 (95%CI: 0.325-0.617), specificity was 0.929 (95%CI: 0.877-0.964), positive predictive value was 0.676 (95%CI: 0.484-0.745), negative predictive value was 0.847 (95%CI: 0.825-0.865).
Conclusion: Compared with the IID, Mallampati classification and ULBT, C-TMD has higher value in predicting difficult laryngoscopy and does not require the exposure of upper respiratory tract.
Trial registration: The study was registered on October 21, 2019 in the Chinese Clinical Trial Registry ( ChiCTR1900026775 ).
Keywords: Airway management; COVID-19 epidemic; Difficult laryngoscopy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures


References
-
- Sullivan P. Anaesthesia for medical students [M] Ottawa: the Department of Anaesthesia, Ottawa Civic Hospital; 1999. p. 35.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
