

Effect of sodium-glucose cotransporter 2 inhibitors on cardiac structure and function in type 2 diabetes mellitus patients with or without chronic heart failure: a meta-analysis
- PMID: 33494751
- PMCID: PMC7836497
- DOI: 10.1186/s12933-020-01209-y
Effect of sodium-glucose cotransporter 2 inhibitors on cardiac structure and function in type 2 diabetes mellitus patients with or without chronic heart failure: a meta-analysis
Abstract
Background: Although the benefits of sodium-glucose cotransporter 2 inhibitors (SGLT2i) on cardiovascular events have been reported in patients with type 2 diabetes mellitus (T2DM) with or without heart failure (HF), the impact of SGLT2i on cardiac remodelling remains to be established.
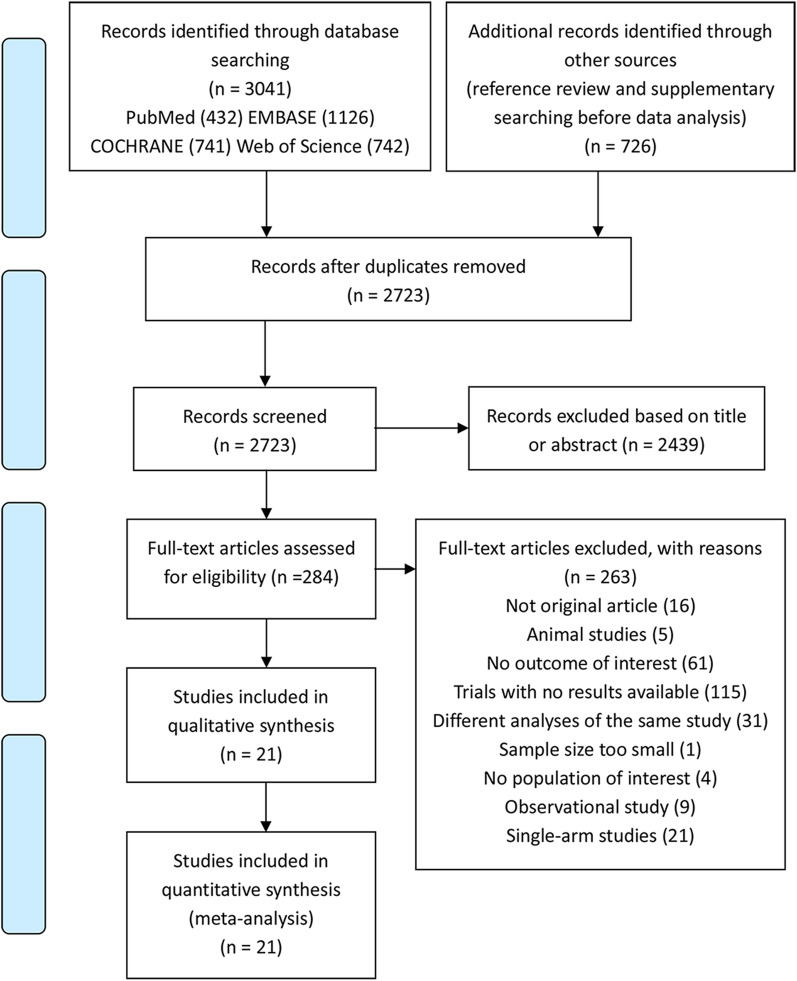
Methods: We searched the PubMed, Embase, Cochrane Library and Web of Science databases up to November 16th, 2020, for randomized controlled trials reporting the effects of SGLT2i on parameters of cardiac structure, cardiac function, plasma N-terminal pro-brain natriuretic peptide (NT-proBNP) level or the Kansas City Cardiomyopathy Questionnaire (KCCQ) score in T2DM patients with or without chronic HF. The effect size was expressed as the mean difference (MD) or standardized mean difference (SMD) and its 95% confidence interval (CI). Subgroup analyses were performed based on the stage A-B or stage C HF population and HF types.
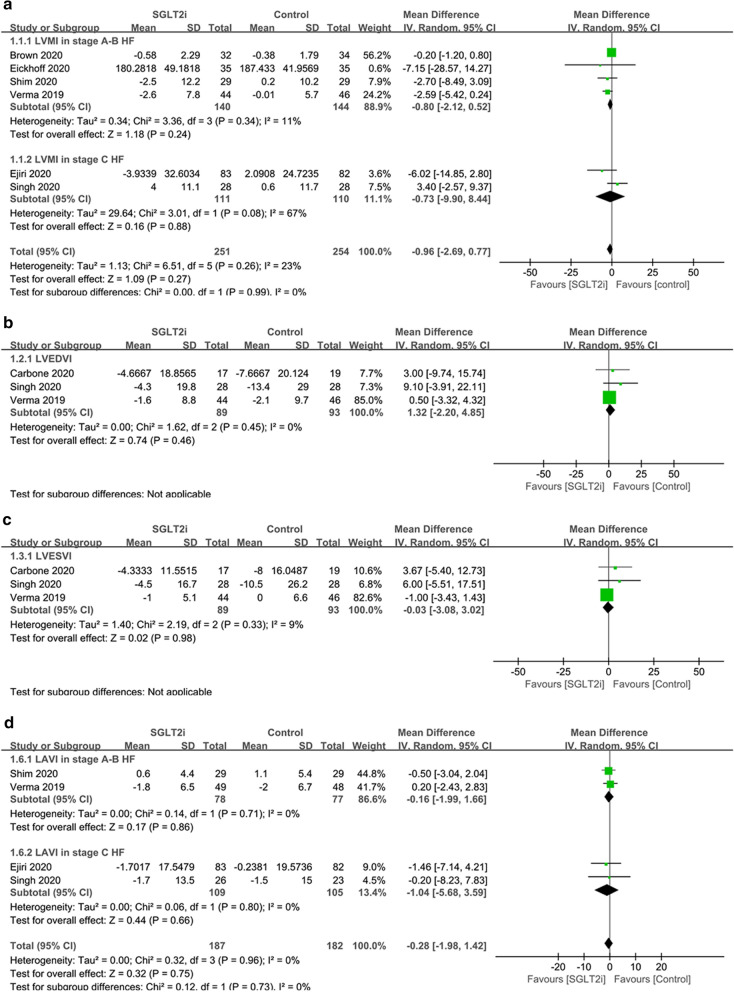
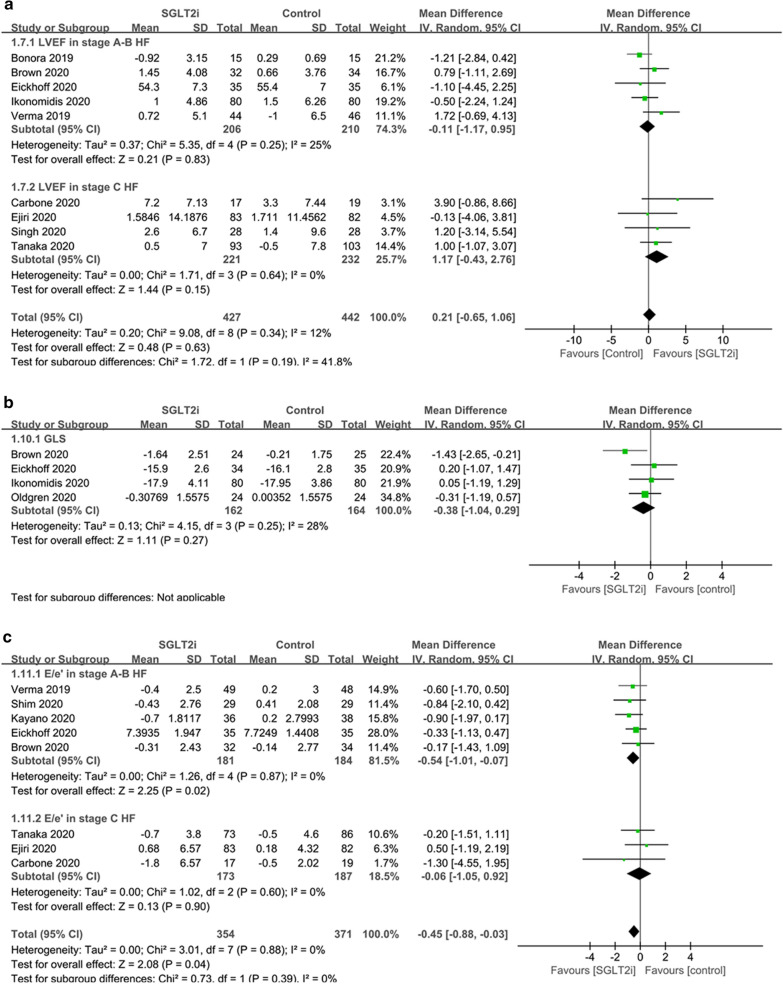
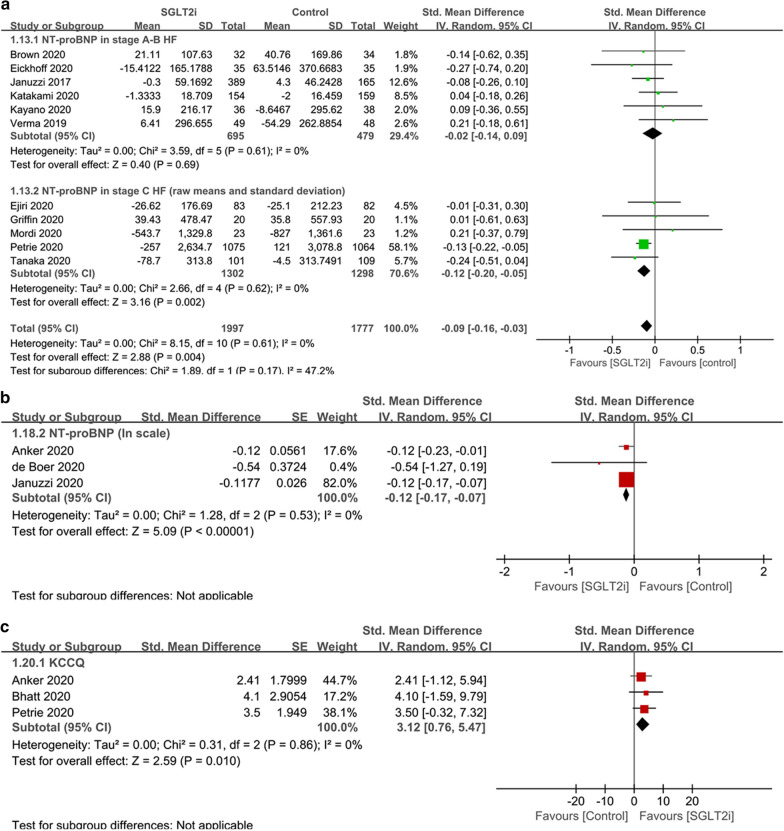
Results: Compared to placebo or other antidiabetic drugs, SGLT2i showed no significant effects on left ventricular mass index, left ventricular end diastolic volume index, left ventricular end systolic volume index, or left atrial volume index. SGLT2i improved left ventricular ejection fraction only in the subgroup of HF patients with reduced ejection fraction (MD 3.16%, 95% CI 0.11 to 6.22, p = 0.04; I2 = 0%), and did not affect the global longitudinal strain in the overall analysis including stage A-B HF patients. SGLT2i showed benefits in the E/e' ratio (MD - 0.45, 95% CI - 0.88 to - 0.03, p = 0.04; I2 = 0%), plasma NT-proBNP level (SMD - 0.09, 95% CI - 0.16 to - 0.03, p = 0.004; I2 = 0%), and the KCCQ score (SMD 3.12, 95% CI 0.76 to 5.47, p = 0.01; I2 = 0%) in the overall population.
Conclusion: The use of SGLT2i was associated with significant improvements in cardiac diastolic function, plasma NT-proBNP level, and the KCCQ score in T2DM patients with or without chronic HF, but did not significantly affect cardiac structural parameters indexed by body surface area. The LVEF level was improved only in HF patients with reduced ejection fraction.
Keywords: Cardiac remodelling; Chronic heart failure; Sodium–glucose cotransporter 2 inhibitors; Type 2 diabetes mellitus.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Effect of sodium-glucose cotransporter-2 inhibitors on cardiac remodelling: a systematic review and meta-analysis.Eur J Prev Cardiol. 2022 Feb 3;28(17):1961-1973. doi: 10.1093/eurjpc/zwab173. Eur J Prev Cardiol. 2022. PMID: 34792124
-
Effects of canagliflozin on NT-proBNP stratified by left ventricular diastolic function in patients with type 2 diabetes and chronic heart failure: a sub analysis of the CANDLE trial.Cardiovasc Diabetol. 2021 Sep 14;20(1):186. doi: 10.1186/s12933-021-01380-w. Cardiovasc Diabetol. 2021. PMID: 34521417 Free PMC article. Clinical Trial.
-
Long-term surrogate cardiovascular outcomes of SGLT2 inhibitor empagliflozin in chronic heart failure: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2024 Nov 22;24(1):663. doi: 10.1186/s12872-024-04316-w. BMC Cardiovasc Disord. 2024. PMID: 39578752 Free PMC article.
-
Effects of antidiabetic drugs on left ventricular function/dysfunction: a systematic review and network meta-analysis.Cardiovasc Diabetol. 2020 Jan 22;19(1):10. doi: 10.1186/s12933-020-0987-x. Cardiovasc Diabetol. 2020. PMID: 31969144 Free PMC article.
-
Positive effect of dapagliflozin on left ventricular longitudinal function for type 2 diabetic mellitus patients with chronic heart failure.Cardiovasc Diabetol. 2020 Jan 7;19(1):6. doi: 10.1186/s12933-019-0985-z. Cardiovasc Diabetol. 2020. PMID: 31910853 Free PMC article.
Cited by
-
Effect of canagliflozin on N-terminal pro-brain natriuretic peptide in patients with type 2 diabetes and chronic heart failure according to baseline use of glucose-lowering agents.Cardiovasc Diabetol. 2021 Sep 3;20(1):175. doi: 10.1186/s12933-021-01369-5. Cardiovasc Diabetol. 2021. PMID: 34479543 Free PMC article. Clinical Trial.
-
YuNü-Jian attenuates diabetes-induced cardiomyopathy: integrating network pharmacology and experimental validation.Front Endocrinol (Lausanne). 2023 May 23;14:1195149. doi: 10.3389/fendo.2023.1195149. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37288289 Free PMC article.
-
Empagliflozin improves left ventricular ejection fraction and end systolic volume in patients with type 2 diabetes mellitus and coronary artery disease: a post-hoc analysis of EMPA-CARD trial.J Diabetes Metab Disord. 2024 Mar 7;23(1):1107-1111. doi: 10.1007/s40200-024-01393-8. eCollection 2024 Jun. J Diabetes Metab Disord. 2024. PMID: 38932825 Free PMC article.
-
Reduction of cardiac adipose tissue volume with short-term empagliflozin treatment in patients with type 2 diabetes: A substudy from the SIMPLE randomized clinical trial.Diabetes Obes Metab. 2023 Mar;25(3):844-855. doi: 10.1111/dom.14933. Epub 2023 Jan 3. Diabetes Obes Metab. 2023. PMID: 36484428 Free PMC article. Clinical Trial.
-
Association between Dapagliflozin, Cardiac Biomarkers and Cardiac Remodeling in Patients with Diabetes Mellitus and Heart Failure.Life (Basel). 2023 Aug 20;13(8):1778. doi: 10.3390/life13081778. Life (Basel). 2023. PMID: 37629635 Free PMC article.
References
-
- MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J. 2008;29(11):1377–1385. doi: 10.1093/eurheartj/ehn153. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
