

Management of Heart Failure Patient with CKD
- PMID: 33495289
- PMCID: PMC8425606
- DOI: 10.2215/CJN.14180920
Management of Heart Failure Patient with CKD
Abstract
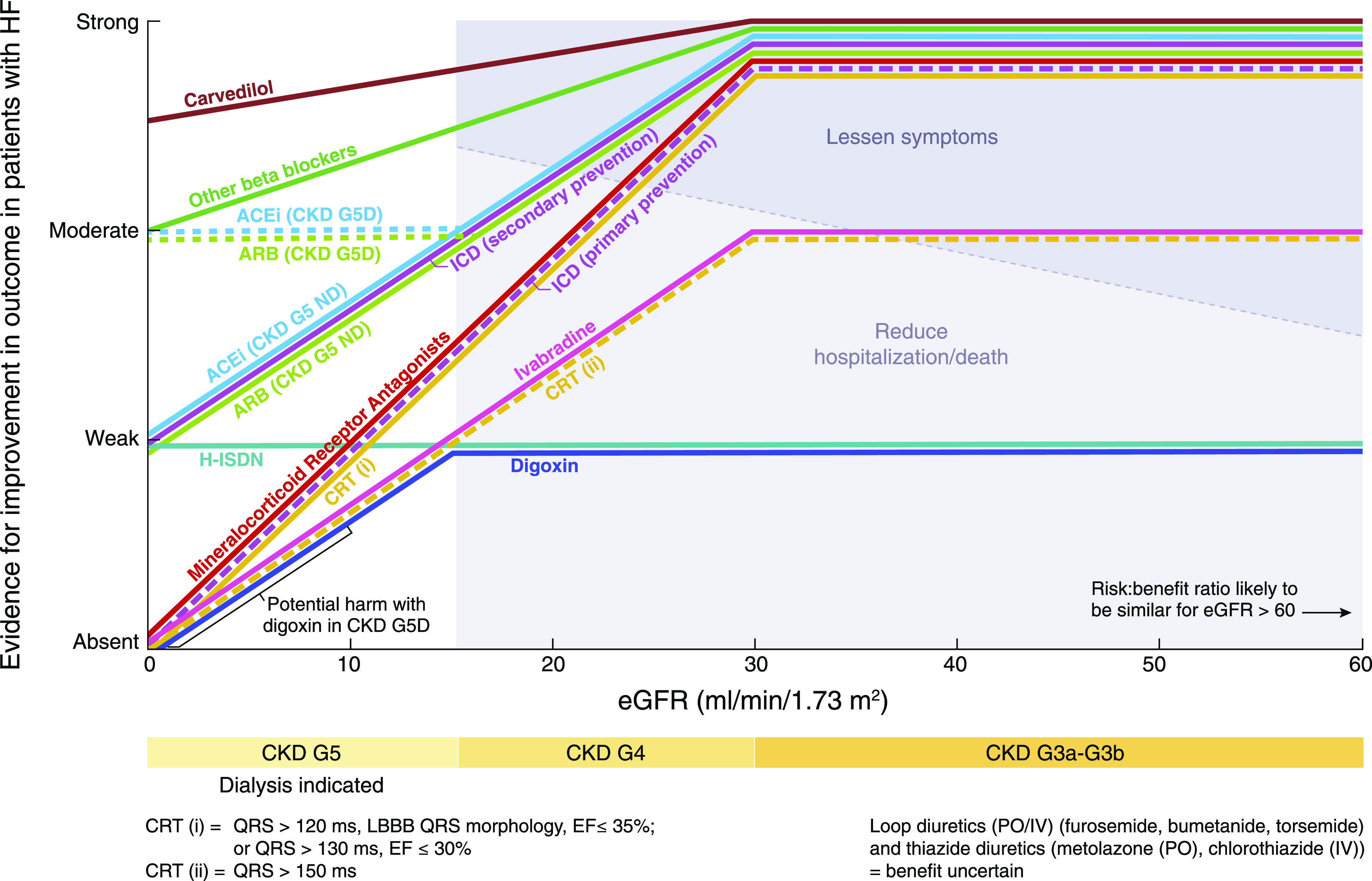
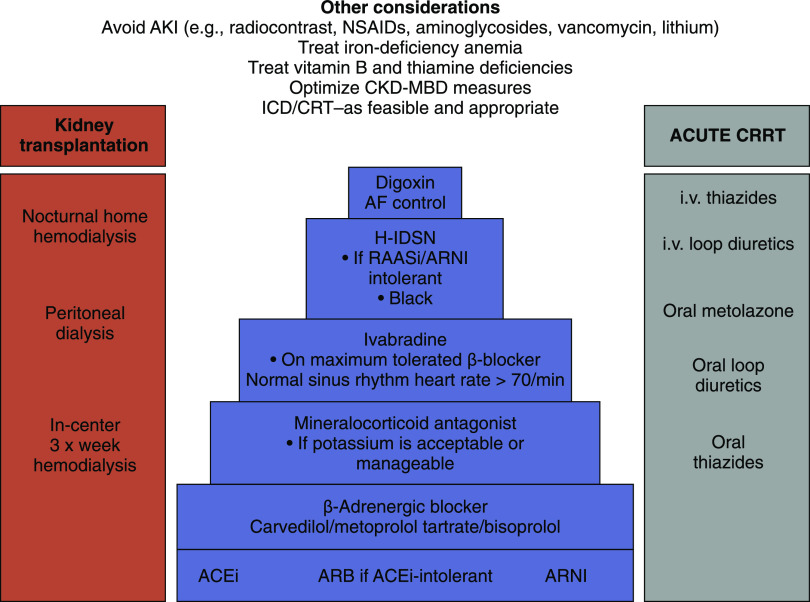
CKD is common in patients with heart failure, associated with high mortality and morbidity, which is even higher in people undergoing long-term dialysis. Despite increasing use of evidence-based drug and device therapy in patients with heart failure in the general population, patients with CKD have not benefitted. This review discusses prevalence and evidence of kidney replacement, device, and drug therapies for heart failure in CKD. Evidence for treatment with β-blockers, angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, angiotensin receptor neprilysin inhibitors, and sodium-glucose cotransporter inhibitors in mild-to-moderate CKD has emerged from general population studies in patients with heart failure with reduced ejection fraction (HFrEF). β-Blockers have been shown to improve outcomes in patients with HFrEF in all stages of CKD, including patients on dialysis. However, studies of HFrEF selected patients with creatinine <2.5 mg/dl for ACE inhibitors, <3.0 mg/dl for angiotensin-receptor blockers, and <2.5 mg/dl for mineralocorticoid receptor antagonists, excluding patients with severe CKD. Angiotensin receptor neprilysin inhibitor therapy was successfully used in randomized trials in patients with eGFR as low as 20 ml/min per 1.73 m2 Hence, the benefits of renin-angiotensin-aldosterone axis inhibitor therapy in patients with mild-to-moderate CKD have been demonstrated, yet such therapy is not used in all suitable patients because of fear of hyperkalemia and worsening kidney function. Sodium-glucose cotransporter inhibitor therapy improved mortality and hospitalization in patients with HFrEF and CKD stages 3 and 4 (eGFR>20 ml/min per 1.73 m2). High-dose and combination diuretic therapy, often necessary, may be complicated with worsening kidney function and electrolyte imbalances, but has been used successfully in patients with CKD stages 3 and 4. Intravenous iron improved symptoms in patients with heart failure and CKD stage 3; and high-dose iron reduced heart failure hospitalizations by 44% in patients on dialysis. Cardiac resynchronization therapy reduced death and hospitalizations in patients with heart failure and CKD stage 3. Peritoneal dialysis in patients with symptomatic fluid overload improved symptoms and prevented hospital admissions. Evidence suggests that combined cardiology-nephrology clinics may help improve management of patients with HFrEF and CKD. A multidisciplinary approach may be necessary for implementation of evidence-based therapy.
Keywords: chronic kidney disease; dialysis; heart failure.
Copyright © 2021 by the American Society of Nephrology.
Figures
References
-
- House AA, Wanner C, Sarnak MJ, Piña IL, McIntyre CW, Komenda P, Kasiske BL, Deswal A, deFilippi CR, Cleland JGF, Anker SD, Herzog CA, Cheung M, Wheeler DC, Winkelmayer WC, McCullough PA; Conference Participants: Heart failure in chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 95: 1304–1317, 2019 - PubMed
-
- Damman K, Valente MA, Voors AA, O’Connor CM, van Veldhuisen DJ, Hillege HL: Renal impairment, worsening renal function, and outcome in patients with heart failure: An updated meta-analysis. Eur Heart J 35: 455–469, 2014 - PubMed
-
- Kottgen A, Russell SD, Loehr LR, Crainiceanu CM, Rosamond WD, Chang PP, Chambless LE, Coresh J: Reduced kidney function as a risk factor for incident heart failure: The Atherosclerosis Risk in Communities (ARIC) study. J Am Soc Nephrol 18: 1307–1315, 2007 - PubMed
-
- Amsalem Y, Garty M, Schwartz R, Sandach A, Behar S, Caspi A, Gottlieb S, Ezra D, Lewis BS, Leor J: Prevalence and significance of unrecognized renal insufficiency in patients with heart failure. Eur Heart J 29: 1029–1036, 2008 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
