

Natural History, Phenotypic Spectrum, and Discriminative Features of Multisystemic RFC1 Disease
- PMID: 33495376
- PMCID: PMC8055326
- DOI: 10.1212/WNL.0000000000011528
Natural History, Phenotypic Spectrum, and Discriminative Features of Multisystemic RFC1 Disease
Abstract
Objective: To delineate the full phenotypic spectrum, discriminative features, piloting longitudinal progression data, and sample size calculations of replication factor complex subunit 1 (RFC1) repeat expansions, recently identified as causing cerebellar ataxia, neuropathy, vestibular areflexia syndrome (CANVAS).
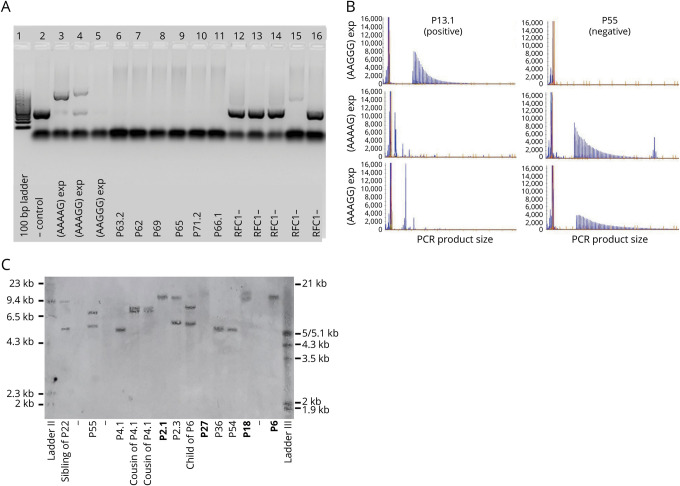
Methods: Multimodal RFC1 repeat screening (PCR, Southern blot, whole-exome/genome sequencing-based approaches) combined with cross-sectional and longitudinal deep phenotyping in (1) cross-European cohort A (70 families) with ≥2 features of CANVAS or ataxia with chronic cough (ACC) and (2) Turkish cohort B (105 families) with unselected late-onset ataxia.
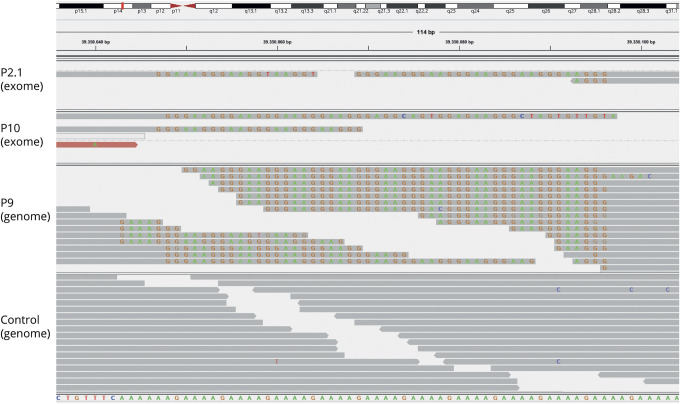
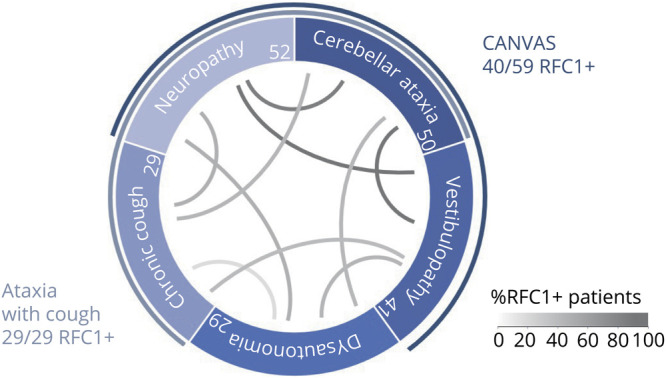
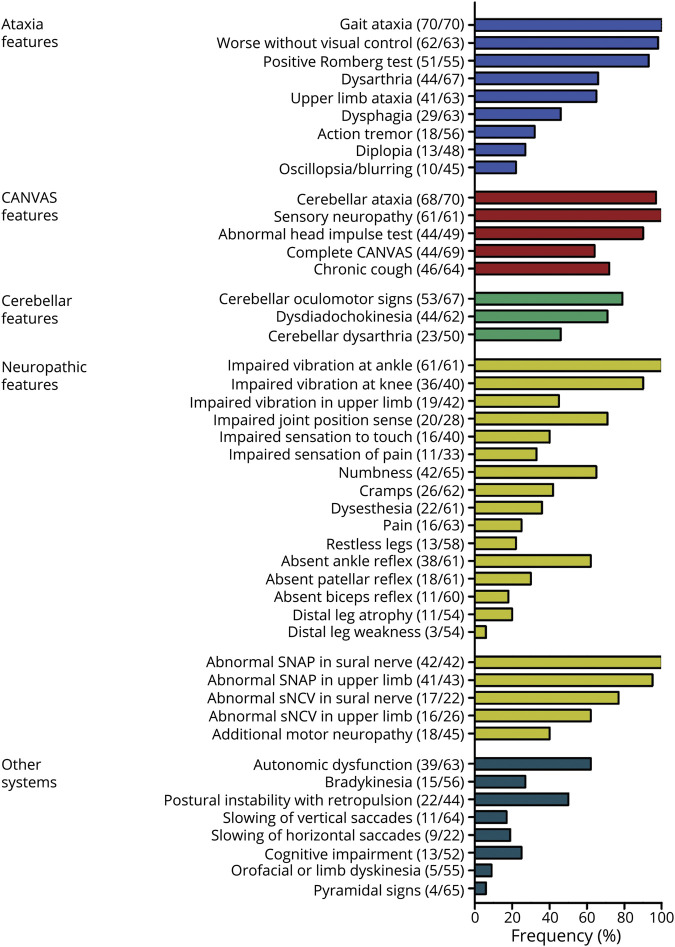
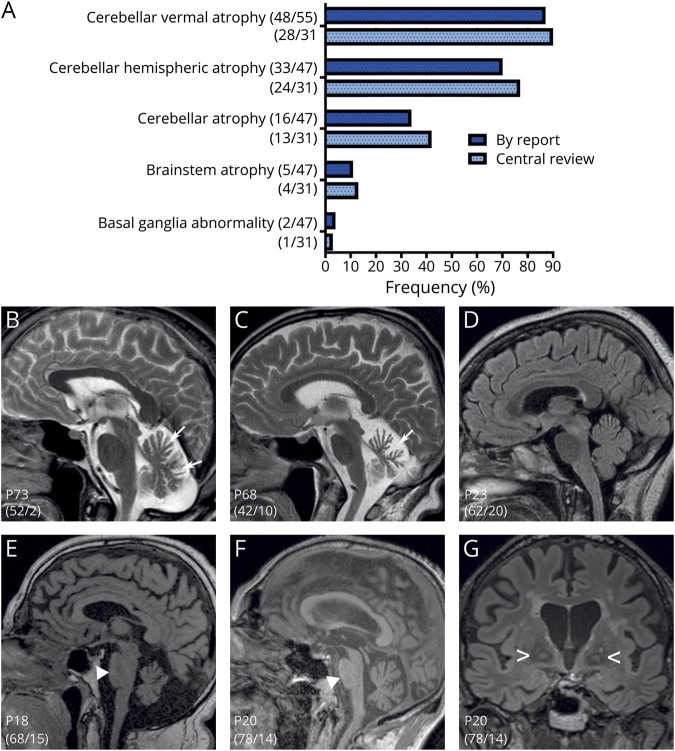
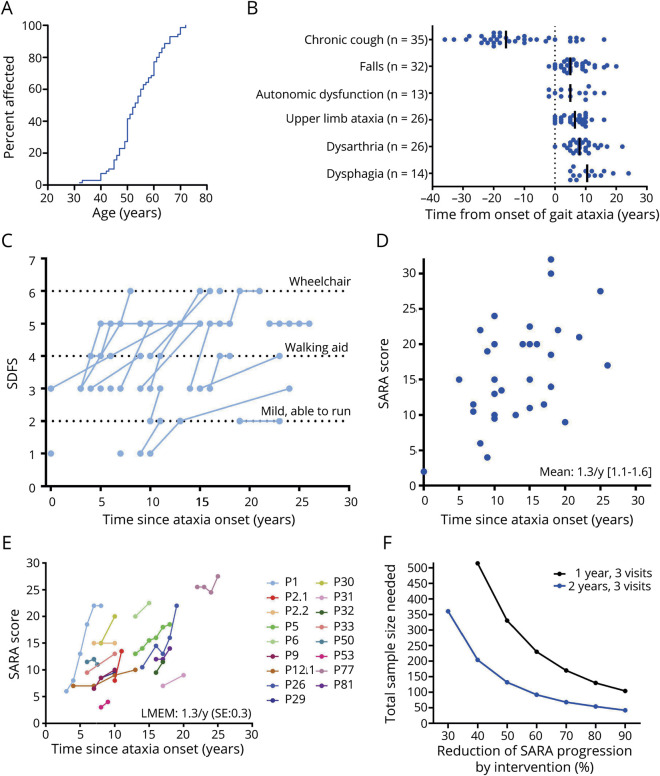
Results: Prevalence of RFC1 disease was 67% in cohort A, 14% in unselected cohort B, 68% in clinical CANVAS, and 100% in ACC. RFC1 disease was also identified in Western and Eastern Asian individuals and even by whole-exome sequencing. Visual compensation, sensory symptoms, and cough were strong positive discriminative predictors (>90%) against RFC1-negative patients. The phenotype across 70 RFC1-positive patients was mostly multisystemic (69%), including dysautonomia (62%) and bradykinesia (28%) (overlap with cerebellar-type multiple system atrophy [MSA-C]), postural instability (49%), slow vertical saccades (17%), and chorea or dystonia (11%). Ataxia progression was ≈1.3 Scale for the Assessment and Rating of Ataxia points per year (32 cross-sectional, 17 longitudinal assessments, follow-up ≤9 years [mean 3.1 years]) but also included early falls, variable nonlinear phases of MSA-C-like progression (SARA points 2.5-5.5 per year), and premature death. Treatment trials require 330 (1-year trial) and 132 (2-year trial) patients in total to detect 50% reduced progression.
Conclusions: RFC1 disease is frequent and occurs across continents, with CANVAS and ACC as highly diagnostic phenotypes yet as variable, overlapping clusters along a continuous multisystemic disease spectrum, including MSA-C-overlap. Our natural history data help to inform future RFC1 treatment trials.
Classification of evidence: This study provides Class II evidence that RFC1 repeat expansions are associated with CANVAS and ACC.
Copyright © 2021 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the American Academy of Neurology.
Figures
References
-
- Szmulewicz DJ, McLean CA, MacDougall HG, Roberts L, Storey E, Halmagyi GM. CANVAS an update: clinical presentation, investigation and management. J Vestib Res 2014;24:465–474. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials