

Common genetic variants and modifiable risk factors underpin hypertrophic cardiomyopathy susceptibility and expressivity
- PMID: 33495597
- PMCID: PMC8240954
- DOI: 10.1038/s41588-020-00764-0
Common genetic variants and modifiable risk factors underpin hypertrophic cardiomyopathy susceptibility and expressivity
Abstract
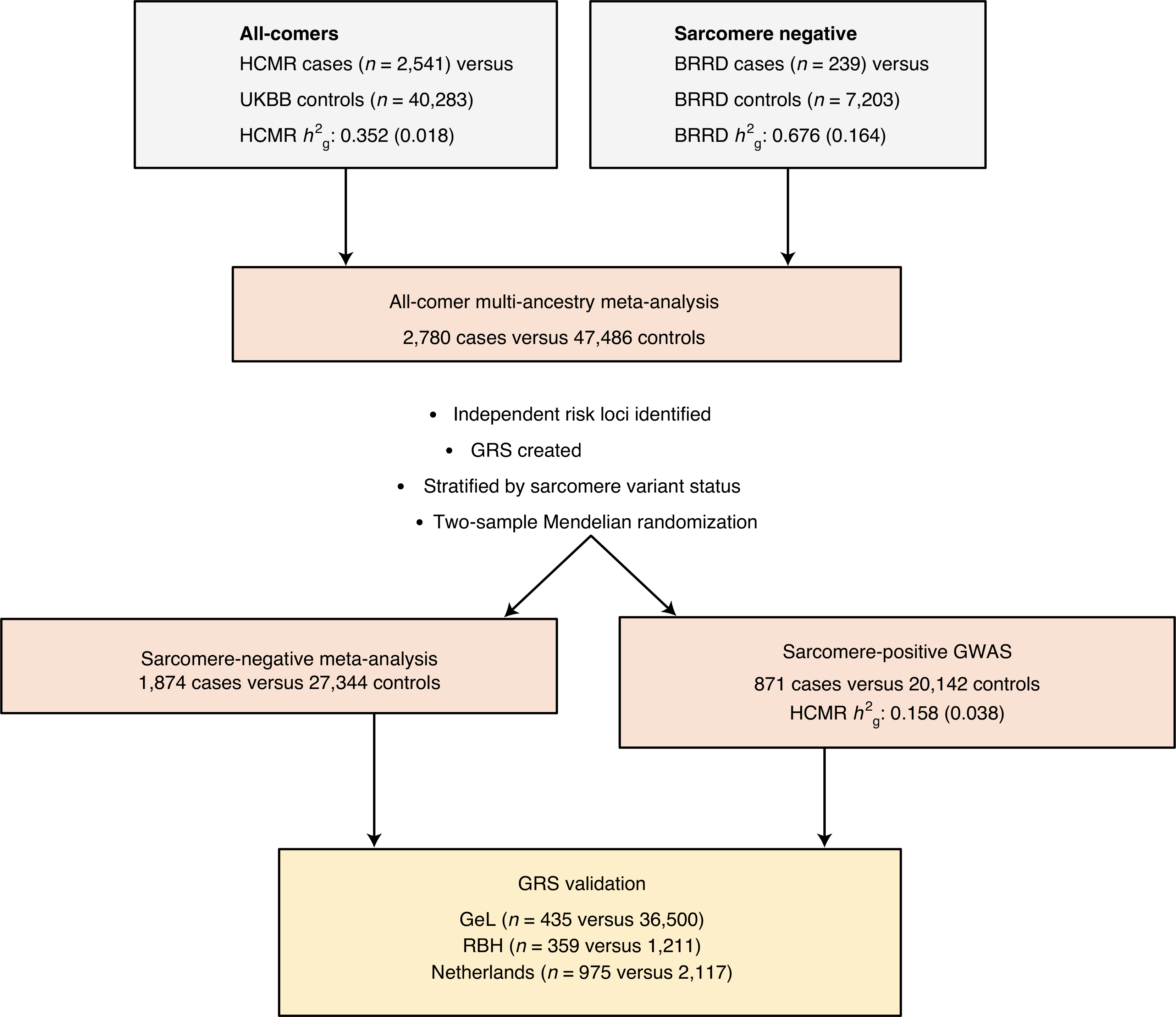
Hypertrophic cardiomyopathy (HCM) is a common, serious, genetic heart disorder. Rare pathogenic variants in sarcomere genes cause HCM, but with unexplained phenotypic heterogeneity. Moreover, most patients do not carry such variants. We report a genome-wide association study of 2,780 cases and 47,486 controls that identified 12 genome-wide-significant susceptibility loci for HCM. Single-nucleotide polymorphism heritability indicated a strong polygenic influence, especially for sarcomere-negative HCM (64% of cases; h2g = 0.34 ± 0.02). A genetic risk score showed substantial influence on the odds of HCM in a validation study, halving the odds in the lowest quintile and doubling them in the highest quintile, and also influenced phenotypic severity in sarcomere variant carriers. Mendelian randomization identified diastolic blood pressure (DBP) as a key modifiable risk factor for sarcomere-negative HCM, with a one standard deviation increase in DBP increasing the HCM risk fourfold. Common variants and modifiable risk factors have important roles in HCM that we suggest will be clinically actionable.
Conflict of interest statement
Competing interests
As of April 2020, A.R.H. is an employee of AstraZeneca.
Figures



Comment in
-
New insights into the genetics of cardiomyopathies.Nat Rev Cardiol. 2021 Apr;18(4):229. doi: 10.1038/s41569-021-00526-3. Nat Rev Cardiol. 2021. PMID: 33564142 No abstract available.
References
-
- Yotti R, Seidman CE & Seidman JG Advances in the genetic basis and pathogenesis of sarcomere cardiomyopathies. Annu. Rev. Genomics Hum. Genet. 20, 129–153 (2019). - PubMed
-
- Harper AR, Parikh VN, Goldfeder RL, Caleshu C & Ashley EA Delivering clinical grade sequencing and genetic test interpretation for cardiovascular medicine. Circ. Cardiovasc. Genet. 10, e001221 (2017). - PubMed
-
- Watkins H, Ashrafian H & Redwood C Inherited cardiomyopathies. N. Engl. J. Med. 364, 1643–1656 (2011). - PubMed
-
- Ingles J et al. Nonfamilial hypertrophic cardiomyopathy: prevalence, natural history and clinical implication. Circ. Cardiovasc. Genet 10, e001620 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- 203141/WT_/Wellcome Trust/United Kingdom
- RG/18/9/33887/BHF_/British Heart Foundation/United Kingdom
- 090532/Z/09/Z/WT_/Wellcome Trust/United Kingdom
- 1964807/MRC_/Medical Research Council/United Kingdom
- RE/13/1/30181/BHF_/British Heart Foundation/United Kingdom
- MC_UP_1102/20/MRC_/Medical Research Council/United Kingdom
- 090532/WT_/Wellcome Trust/United Kingdom
- U01 HL117006/HL/NHLBI NIH HHS/United States
- 201543/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- CRUK_/Cancer Research UK/United Kingdom
- 203141/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- DH_/Department of Health/United Kingdom
- 201543/B/16/Z/WT_/Wellcome Trust/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
