

Life expectancy and mortality in 363 cities of Latin America
- PMID: 33495602
- PMCID: PMC7960508
- DOI: 10.1038/s41591-020-01214-4
Life expectancy and mortality in 363 cities of Latin America
Abstract
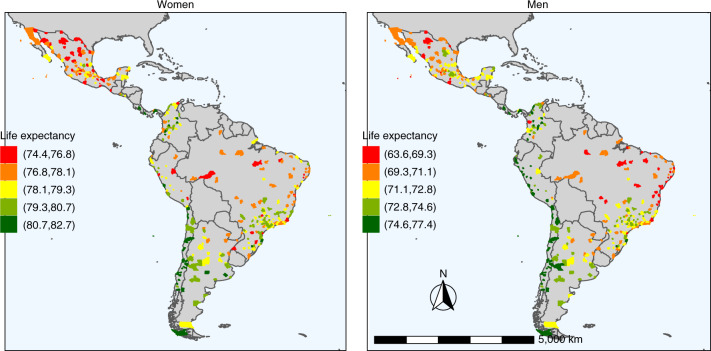
The concept of a so-called urban advantage in health ignores the possibility of heterogeneity in health outcomes across cities. Using a harmonized dataset from the SALURBAL project, we describe variability and predictors of life expectancy and proportionate mortality in 363 cities across nine Latin American countries. Life expectancy differed substantially across cities within the same country. Cause-specific mortality also varied across cities, with some causes of death (unintentional and violent injuries and deaths) showing large variation within countries, whereas other causes of death (communicable, maternal, neonatal and nutritional, cancer, cardiovascular disease and other noncommunicable diseases) varied substantially between countries. In multivariable mixed models, higher levels of education, water access and sanitation and less overcrowding were associated with longer life expectancy, a relatively lower proportion of communicable, maternal, neonatal and nutritional deaths and a higher proportion of deaths from cancer, cardiovascular disease and other noncommunicable diseases. These results highlight considerable heterogeneity in life expectancy and causes of death across cities of Latin America, revealing modifiable factors that could be amenable to urban policies aimed toward improving urban health in Latin America and more generally in other urban environments.
Conflict of interest statement
The authors declare no competing interests.
Figures













Comment in
-
Understanding life and death in Latin America.Nat Med. 2021 Mar;27(3):373-375. doi: 10.1038/s41591-021-01277-x. Nat Med. 2021. PMID: 33664489 No abstract available.
References
-
- UNDP Population Division. World Urbanization Prospects: The 2018 Revisionhttps://population.un.org/wup/ (2018).
-
- UN-HABITAT. Urbanization and Development: Emerging Futures; World Cities Report 2016 (UN-HABITAT, 2016).
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
